Original
Analysis of the PHQ-15 by individual items: a systematic review and meta-analysis
Oleksandr Boiko (a, Sara Barrio-Martínez (b, c, Amador Priede (b,d, Ludovica Ventura (b, Nerea Gómez-Carazo (e, Aida Hernández-Abellán (e, Esther Setién-Suero (b, César González-Blanch (b,e
- Unidad de Formación, Docencia e Investigación. Gerencia de Atención Primaria. Santander, (España)
- Facultad de Psicología, Universidad Complutense de Madrid, España. Instituto de Investigación Sanitaria Marqués de Valdecilla (IDIVAL), Santander, (España)
- Facultad de Psicología. Universidad Complutense de Madrid. Madrid, (España)
- Unidad de Salud Mental. Hospital de Laredo, Laredo, (España)
- Unidad de Salud Mental “Puertochico”, Hospital Universitario Marqués de Valdecilla, Santander, (España)
Ansiedad y Estrés, 28, (2022), 62-73
https://doi.org/10.5093/anyes2022a7
https://www.ansiedadyestres.es
Bibliography reference
INFO ARTICLE
Recibido el 10 de junio de 2021
Aceptado el 12 de agosto de 2021
Online el 21 de diciembre de 2021
ABSTRACT
Background: The Patient Health Questionnaire-15 (PHQ-15) is among the most commonly used questionnaires to assess somatic symptoms in primary care settings. The aim of our study was to conduct a systematic review and meta-analysis of the studies that have analysed individual items from the PHQ-15 to determine the influence of differences in sociodemographic and clinical variables.
Methods: This systematic review was conducted in accordance with the PRISMA statement. Studies analysing PHQ-15 by individual items were searched in Medline/PubMed, Embase, PsycINFO, Scopus from 1999 to November 2019.
Results: Data were extracted from 13 studies. The most frequently reported symptoms were "pain in your arms, legs, or joints", "back pain", "headaches", and "feeling tired or having low energy". In patients with mental health disorders (depression, anxiety disorder, and somatoform disorder), the most commonly reported somatic symptoms were "trouble sleeping", "feeling tired or having low energy", and digestive symptoms. In the meta-analysis, females scored significantly higher than males on 3 of 14 items: "headaches" (odds ratio [OR] 2.16, p<.001), "dizziness" (OR 1.58, p<.001), and "stomach pain" (OR 1.46, p<.02), with a small to moderate effect size for these differences.
Conclusions: Gender differences were detected for three items (headaches, dizziness, and stomach pain), although the magnitude of these differences was small. Further research is needed to better understand the relationship between individual items and other sociodemographic variables. In addition, more research is needed to determine measurement invariance across various demographic groups.
KEYWORDS
PHQ-15
Functional Somatic Symptoms
Somatization
Patient Health Questionnaire
Gender differences
Análisis del PHQ-15 por ítems individuales: revisión sistemática y metaanálisis
Ansiedad y Estrés, 28, (2022), 62-73
https://doi.org/10.5093/anyes2022a7
https://www.ansiedadyestres.es
Bibliography reference
RESUMEN
Introducción: El PHQ-15 (Patient Health Questionnaire) es uno de los cuestionarios más utilizados para la valoración de los síntomas somáticos en atención primaria. El objetivo del estudio fue realizar una revisión sistemática y un metaanálisis de los estudios previos que analizaron los ítems individuales del PHQ-15 y determinar su asociación con las variables clínicas y sociodemográficas.
Metodología: Esta revisión sistemática se llevó a cabo de acuerdo a la declaración PRISMA. Los estudios que analizaron el PHQ-15 por ítems individuales fueron obtenidos en las bases de datos de Medline / PubMed, Embase, PsycINFO y Scopus; desde el 1999 hasta noviembre de 2019.
Resultados: Los datos fueron extraídos de 13 estudios. Los síntomas más frecuentes fueron "dolor en los brazos, piernas o articulaciones", "dolor de espalda", "dolor de cabeza" y "sentirse cansado o con poca energía". Los pacientes con trastornos mentales (depresión, ansiedad y trastorno somatomorfo), presentaron con mayor frecuencia "problemas de sueño", "sentirse cansado o con poca energía" y síntomas gastrointestinales. En el metaanálisis, las mujeres obtuvieron puntuaciones significativamente mayores que los hombres en 3 de los 14 ítems: "dolor de cabeza" (odds ratio [OR] 2.16, p<.001), "mareo" (OR 1.58, p<.001) y "dolor de estómago" (OR 1.46, p<0,02), con un tamaño del efecto de pequeño a moderado.
Conclusiones: Se detectaron diferencias entre ambos géneros en tres ítems (cefalea, mareo y dolor de estómago), aunque la magnitud de estas diferencias fue pequeña. Es necesario seguir investigando para lograr una mejor comprensión de la relación entre los ítems individuales y las variables sociodemográficas. Además, es necesario investigar la invarianza de medición en los diferentes grupos demográficos.
PALABRAS CLAVE
PHQ-15
Síntomas somáticos funcionales
Somatización
Patient Health Questionnaire
Diferencias de género
INTRODUCTION
Functional somatic symptoms (FSS)—also called ‘medically unexplained symptoms’, ‘somatisation’, ‘somatoform’, or ‘bodily distress’ symptoms—are those symptoms that cannot be fully explained or attributed to a specific organic disease (Marks and Hunter, 2015). These symptoms are difficult to treat due to their nonspecific cause and their prevalence in the general population is associated with numerous health-related issues and high health care costs (Henningsen et al., 2007). FSS are common in general medical care settings, with a prevalence of up to 30% depending on the diagnostic criteria (Kocalevent et al., 2013, De Waal et al., 2004, Roca et al., 2009). The use of inpatient and outpatient services and annual medical care costs in patients with FSS is twice that of patients without FSS (Barsky et al., 2005). Moreover, the prevalence of FSS in patients with mental disorders is significantly higher than in the general population, showing a strong association with depression and anxiety (Shidhaye et al., 2013), with more than one-third of patients with depression or anxiety presenting comorbid somatic symptoms (Toft et al., 2005, Fink et al., 2004, Henningsen et al., 2003).
According to some systematic reviews, the Patient Health Questionnaire-15 (PHQ-15) is among the best questionnaires to assess FSS in large-scale studies (Zijlema et al., 2013) and in primary care (Sitnikova et al., 2017). Furthermore, the DSM-5 Workgroup on Somatic Symptom Disorders recommends the PHQ-15 as a useful measurement tool for research and evaluation of somatic symptom severity (American Psychiatric Association, 2013). The PHQ-15 is a short, self-administered, easy-to-use, fully validated scale. It assesses the most common and relevant symptoms and is available in multiple languages (Zijlema et al., 2013). The PHQ-15 is the short version of the Primary Care Evaluation of Mental Disorders (PRIME-MD) diagnostic tool (Spitzer et al., 1999), which was initially designed for use in primary care settings, and subsequently applied to several clinical populations, including patients with mental disorders (Kroenke et al., 2006), cancer (Leonhart et al., 2017, Zhang and Zhang, 2017), neurological diseases (Carson et al., 2015), or other pathological and physiological conditions (Wolfe et al., 2014, Wilkie et al., 2018, Witthöft et al., 2013). The PHQ-15 comprises15 items designed to evaluate the most prevalent somatic symptoms. Respondents are asked to rate the severity of these symptoms on a 3-point scale, as follows: 0 (not bothered at all), 1 (bothered a little), or 2 (bothered a lot), with total score ranging from 0 to 30 (Kroenke et al., 2010). To interpret the results, cut-off scores for mild, moderate, and severe somatic symptoms are 5, 10, and 15 points, respectively (Kroenke et al., 2010). Although most studies that have administered the PHQ-15 to assess FSS have relied primarily on the total score, several studies have associated the prevalence of certain component items with distinct clinical and sociodemographic factors (Morawa et al., 2017, Jordan et al., 2018, Hinz et al., 2017, Carlehed et al., 2017). For example, previous studies have found gender differences on certain items, with a significantly higher prevalence of various types of pain and nausea among women; similarly, the prevalence of pain or problems during sexual intercourse is more common in men (Hinz et al., 2017, Beutel et al., 2019). Studies have also assessed the influence of other variables on the prevalence of specific PHQ-15 items, including migration-related variables (Morawa et al., 2017), socioeconomic status (Hinz et al., 2017), risk of suicidal ideation (Jordan et al., 2018), anxiety and depression disorders (Carlehed et al., 2017), and overweight (Hinz et al., 2017). Nevertheless, Cano-García et al. (2020) confirmed the measurement invariance for gender and age in a sample of primary care patients with emotional disorders, using a 13-item version of the PHQ-15.
While most of the studies reported a strong correlation between the total score of PHQ-15 and such factors as gender, socioeconomic status, quality of life, mental and somatic disorders, etc. (Kroenke et al., 2010, Hinz et al., 2017), evaluation of individual items of PHQ-15 has shown significant variation in the frequency and character of reported somatic symptoms depending on the different internal and external factors (Morawa et al., 2017, Jordan et al., 2018, Hinz et al., 2017, Carlehed et al., 2017). Therefore, the influence of certain sociodemographic variables on the individual items of the PHQ-15 and their real effect on a total score of the PHQ-15 is still unclear. It is likely that comprehensive and structured analysis of these differences can be crucial both for clinical practice and future research. A better understanding of the role of individual items would be useful for the management of somatic symptoms in patients with mental disorders in psychiatry and primary care. To date, no systematic review has been performed to assess PHQ-15 outcomes by its component items. The objective of the present study was to conduct a systematic review and meta-analysis of existing studies that have analysed the individual items of the PHQ-15, the prevalence of the symptoms assessed on those items, and, in particular, their association with sociodemographic and clinical variables.
MATERIALS AND METHODS
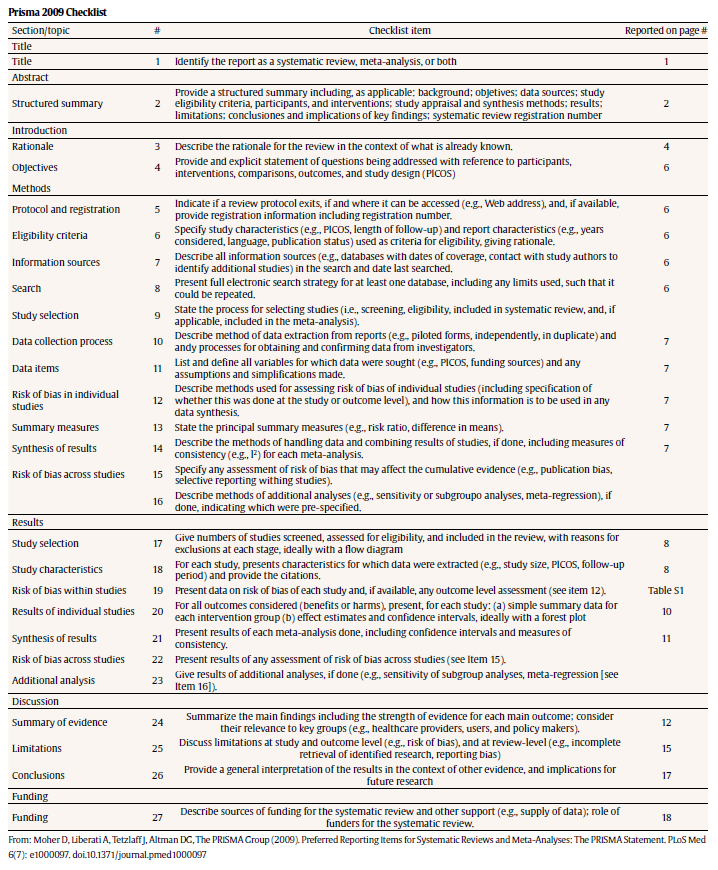
This systematic review is reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines (Liberati et al., 2009) and was pre-registered in PROSPERO (no. CRD42020156660).
Search strategy
We performed a search in the Medline/Pubmed, Embase, PsycINFO, and Scopus databases to identify studies published studies that analysed the PHQ-15 by its individual items. We searched for studies published between 1999 (the year the PHQ was originally published) (Spitzer et al., 1999) and November 2019. The following search term were used: “patient health questionnaire-15” or “patient health questionnaire-13” or “PHQ-15” or “PHQ-13” (several studies use a short version of the PHQ-15 (the PHQ-13). To increase the sensitivity of the search process, all original research articles that contained the relevant search terms were screened by reviewing the full text.
Study selection
To be eligible for inclusion, the primary purpose of the study must have been to evaluate the PHQ-15 by its individual component items in adults with mental disorders (i.e., clinical populations) or the general population if individuals with mental disorders were not excluded. Studies were excluded if they met any of the following criteria: (a) more than 50% of the target population were elderly patients (>70 years old) or patients with pathological conditions or organic disease due to high prevalence and specificity of somatic symptoms in these groups; (b) the study aim was primarily focused on the measurement properties (factor structure, validity, and reliability, etc) of the PHQ-15; c) comments, letters, editorials, book sections, PhD theses, conference publications, and systematic reviews. No language restriction was applied.
The full texts of potentially relevant articles were retrieved and screened for eligibility. Two reviewers (O.B. and S.B.) independently screened the articles for eligibility; disagreements were resolved through discussion. In cases in which the two reviewers could not reach a consensus, a third reviewer (C.G-B.) made the final decision. The result of the selection process is reported in a PRISMA flow diagram (Liberati et al., 2009).
Data extraction
Data extraction was conducted by two authors (O.B. and C.G-B.). The following data were extracted from the included studies: title; first author's name; publication year; country and setting in which the study was performed; participants’ clinical characteristics; sample size; age; language; number of PHQ-15 items; objectives; and results related to analysis of the individual items of the PHQ-15.
Quality assessment
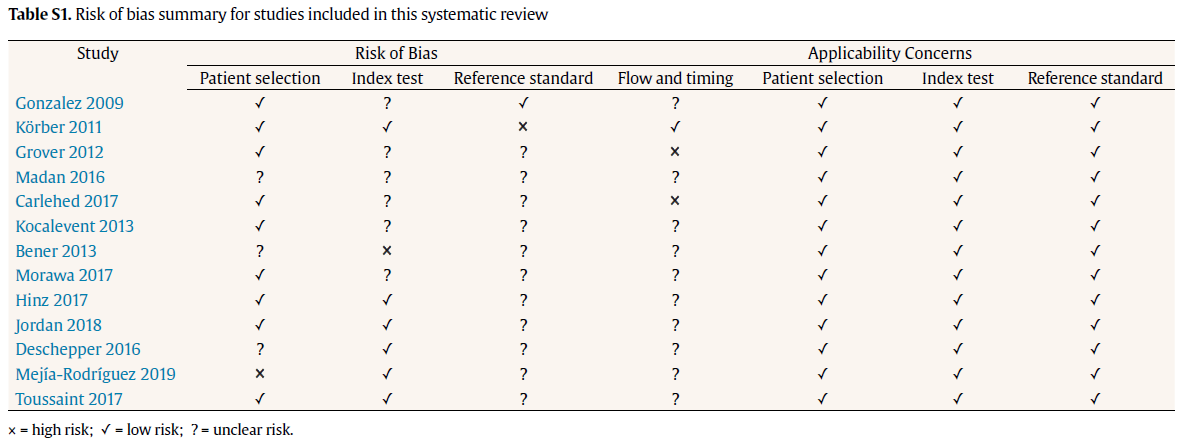
The risk of bias in the included studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) checklist (Whiting et al., 2011) over the following domains: patient selection; index test; reference standard; and flow and timing of the index tests and reference standard. All included studies were assessed for risk of bias in each domain and for applicability concerns in the first three domains. Applicability concerns were rated as “low”, “high”, or “unclear” in terms of how well they matched the review question. This judgement was based on the signalling question: if all questions for one domain were answered “yes”, the risk of bias was rated as “low” (see Table S1). The quality assessment procedure was independently performed by two reviewers (O.B. and S.B.). Discrepancies were resolved by consensus between the two authors and a third reviewer (C.G-B.).
Data synthesis and statistical analysis
For the qualitative synthesis, the main findings from eligible studies were combined narratively using tables of evidence. For the quantitative analysis, odds ratios (OR) and 95% confidence intervals (CI) were used as the primary measure. To account for the expected heterogeneity between studies, a random-effects model was applied for meta-analyses to obtain a combined effect weighted for sample size. The presence of heterogeneity was assessed by calculating the I2 metric and Cochran’s Chi-squared test with I2 > 50% and p < 0.05 indicating statistically significant heterogeneity (i.e., the percentage of between-study variance due to systematic heterogeneity rather than chance). Comprehensive Meta-analysis software (CMA), version 3, was used for all analyses (Borenstein et al., 2013).
RESULTS
Study inclusion
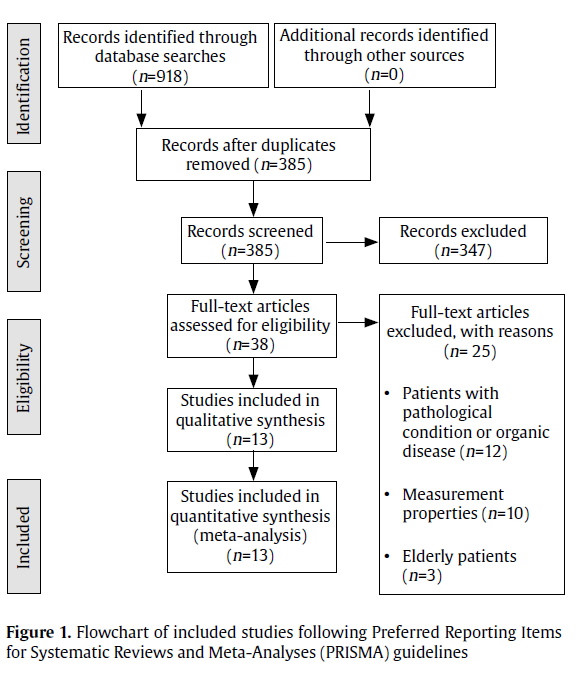
The initial search, including additional sources, detected 918 articles. After discarding duplicates, 385 unique articles were identified. After excluding PhD theses, conference reports, guidelines, and books, 38 articles were selected for full-text screening. Of those, 25 were excluded because they were based on patient samples with organic diseases (Zijlema et al., 2013), studies focused on the psychometric properties of the scale (Fink et al., 2004), and studies involving elderly patients (Kocalevent et al., 2013). Thus, 13 studies were finally included in qualitative synthesis. The selection of studies is summarized in the PRISMA flowchart (Fig. 1).
Figure - 1
Overview of included studies
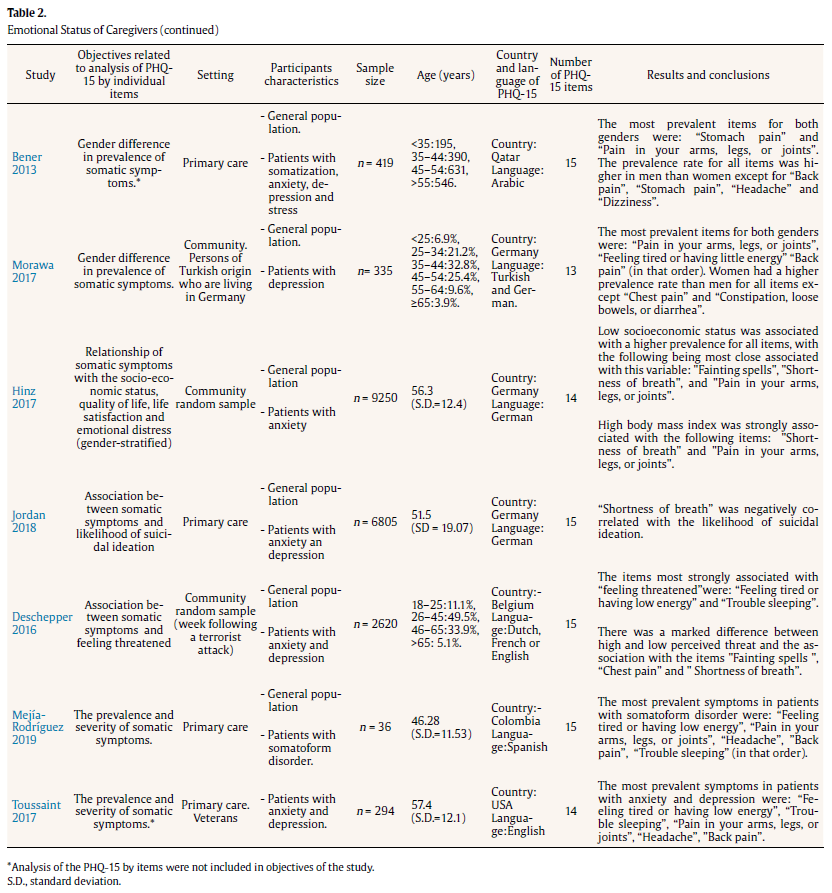
Five studies were conducted in primary care settings (Jordan et al., 2018, Körber et al., 2011, Bener et al., 2013, Mejía-Rodríguez et al., 2019, Toussaint et al., 2017) (Table1). Two studies recruited patients from psychiatry outpatient departments (Gonzalez et al., 2009, Grover et al., 2012) and one from a psychiatric hospital (Madan et al., 2016). Four studies involved community samples (Kocalevent et al., 2013, Hinz et al., 2017, Carlehed et al., 2017, Deschepper et al., 2018) and one study used the PHQ-15 in a community sample of immigrants (Morawa et al., 2017).
Ten studies used the full version of the questionnaire, which consists of either 15 items (for women) or 14 items, excluding the item “menstrual cramps or other problems with your periods” only for men (Jordan et al., 2018, Carlehed et al., 2017, Körber et al., 2011, Bener et al., 2013, Mejía-Rodríguez et al., 2019, Gonzalez et al., 2009, Grover et al., 2012, Madan et al., 2016, Deschepper et al., 2018, Morawa et al., 2017). Two studies used 14 items, excluding the item on menstrual problems (Hinz et al., 2017) o item on sexual problems (Toussaint et al., 2017) for both men and women. One study used only 13 items (PHQ-13), excluding the items “Feeling tired or having low energy” and “Trouble sleeping”, which are also part of the PHQ-9 depression module used in those same studies (Kocalevent et al., 2013).
Overall, the proportion of participants in the studies by gender was balanced, with women accounting for 56.4% and men 43.6% of participants. However, the female/male ratio varied widely, ranging from 12.6% of women in one study (Toussaint et al., 2017) to 94.4% in another (Mejía-Rodríguez et al., 2019). Most studies were based on general population samples (Kocalevent et al., 2013, Morawa et al., 2017, Jordan et al., 2018, Hinz et al., 2017, Carlehed et al., 2017, Körber et al., 2011, Bener et al., 2013, Mejía-Rodríguez et al., 2019, Deschepper et al., 2018). However, two studies assessed samples comprised solely of patients with depression (Gonzalez et al., 2009, Grover et al., 2012), one study included patients with both anxiety and depression (Toussaint et al., 2017), and one involved patients with severe mental disorders (Madan et al., 2016).
The two most commonly reported objectives for the analysis of the individual PHQ-15 items were 1) to investigate the frequency and severity of somatic symptoms (Körber et al., 2011, Mejía-Rodríguez et al., 2019, Toussaint et al., 2017, Grover et al., 2012, Madan et al., 2016) and 2) to analyse gender differences in symptom prevalence rates (Kocalevent et al., 2013, Morawa et al., 2017, Hinz et al., 2017, Bener et al., 2013, Gonzalez et al., 2009). Four studies investigated the association between individual PHQ-15 items and mental health outcomes, such as the risk for anxiety and depression (Carlehed et al., 2017), the likelihood of suicidal ideation (Jordan et al., 2018), socioeconomic status, quality of life, life satisfaction, and emotional distress (Hinz et al., 2017), and feeling threatened and subjective health after a terrorist attack (Deschepper et al., 2018). Three studies evaluated the frequency of somatic symptoms (Toussaint et al., 2017, Madan et al., 2016), including gender stratification (Bener et al., 2013), although this was not specified in the study aims.
Table -2
Study outcomes
Based on the studies that analysed symptom prevalence, the most frequent symptoms were, “pain in your arms, legs, or joints” (Kocalevent et al., 2013, Morawa et al., 2017, Körber et al., 2011, Bener et al., 2013, Mejía-Rodríguez et al., 2019, Toussaint et al., 2017, Gonzalez et al., 2009, Grover et al., 2012), “back pain” (Kocalevent et al., 2013, Morawa et al., 2017, Körber et al., 2011, Bener et al., 2013, Mejía-Rodríguez et al., 2019, Toussaint et al., 2017, Gonzalez et al., 2009), “headaches” (Kocalevent et al., 2013, Morawa et al., 2017, Mejía-Rodríguez et al., 2019, Gonzalez et al., 2009, Grover et al., 2012), and “feeling tired or having low energy” (Morawa et al., 2017, Körber et al., 2011, Mejía-Rodríguez et al., 2019, Toussaint et al., 2017, Grover et al., 2012, Madan et al., 2016).
Figure - 2
In the studies that assessed symptoms in patients with mental health disorders such as depression (Carlehed et al., 2017, Toussaint et al., 2017, Gonzalez et al., 2009, Grover et al., 2012), anxiety disorders (Carlehed et al., 2017, Toussaint et al., 2017), and somatoform disorder (Körber et al., 2011, Mejía-Rodríguez et al., 2019), the most common symptoms were “trouble sleeping”, “feeling tired or having low energy”, and digestive symptoms such as “nausea, gas, or indigestion” and “constipation, loose bowels, or diarrhea”. A study that investigated the relationship between somatic symptoms and the likelihood of suicidal ideation (Jordan et al., 2018) found that “shortness of breath” was contraindicative of suicidal ideation (OR = 0.22).
In the study that investigated the relationship between feeling threatened and subjective health during the week following a terrorist attack (Deschepper et al., 2018), the most frequent symptoms were “feeling tired or having low energy” and “trouble sleeping”. The health-related symptoms that showed the most marked differences between participants with low and high levels of perceived threat were “fainting spells” (OR = 3.6), “chest pain” (OR = 2.4), and “shortness of breath” (OR = 2.4).
Low socioeconomic status was associated with a higher prevalence of all somatic symptoms (Hinz et al., 2017), with the following showing the strongest associations “fainting spells” (OR = 2.91), “shortness of breath” (OR = 2.35), and “pain in your arms, legs, or joints” (OR = 2.04). Obesity was especially associated with “shortness of breath” (OR = 3.35) and “pain in arms, legs, and joints” (OR = 2.34) (Hinz et al., 2017).
Results of gender differences
Four of the five studies that evaluated gender differences found a higher prevalence rate among women for most of the individual items, with women scoring higher than men on 11 to 13 items depending on the study (Kocalevent et al., 2013, Morawa et al., 2017, Hinz et al., 2017, Gonzalez et al., 2009). By contrast, a study conducted in Qatar, men scored higher than women on 10 items (Bener et al., 2013). In two studies, the symptom “pain or problems during sexual intercourse” was more prevalent in men than women: 14.9% vs 12.4% (Gonzalez et al., 2009) and 18.8% vs 12.7% (Hinz et al., 2017). Similarly, in the study by (Kocalevent et al., 2013), “nausea, gas, or indigestion” was more prevalent in men than women (4.6% vs 3.6%). In the study by Morawa et al. (2017), the symptoms “constipation, loose bowels, or diarrhea” (43.3% vs 41.9%) and “chest pain” (35.3% vs 33.2%) were both more prevalent in men. Given these inconsistencies, and the number of studies reporting gender differences, we decided to further explore this by conducting a meta-analysis of those studies (Morawa et al., 2017).
Meta-analysis of gender differences
Four studies were performed in the general population (Kocalevent et al., 2013, Morawa et al., 2017, Hinz et al., 2017, Bener et al., 2013) while one involved patients with major depression (Gonzalez et al., 2009). Of these 5 studies, one was conducted in Spain (Gonzalez et al., 2009), one in Qatar (Bener et al., 2013) and three in Germany (Kocalevent et al., 2013, Morawa et al., 2017, Hinz et al., 2017); however, one of the German studies included only people of Turkish origin (Morawa et al., 2017). The aggregated sample was n = 16 199, of which 56.5% were female.
DISCUSSION
In our narrative summary of the studies, we found that the most prevalent somatic symptoms were those related to pain in the limbs, back, head and fatigue. Mental health problems were associated with higher odds of presenting several somatic symptoms, including sleeping problems, fatigue, and digestive complaints. Low socioeconomic status was associated with a higher prevalence of all somatic symptoms, although this finding was based on only a single study. The main finding of the quantitative analysis was that women experienced more headaches, dizziness, and stomach pain than men.
Heterogeneity among the included studies was high, probably reflecting variability in the study populations assessed in the individual studies (9 of the 13 studies were conducted in the general population while the remaining 4 involved patients with specific mental health disorders), variations in languages and cultures (the studies were performed in 4 continents using the PHQ-15 in nine different languages) and the version of the PHQ-15 used (most studies included all 15 items, but several studies used versions comprised of 14 or 13 items).
Table - 1
The studies can be classified into three groups according to the objectives related to the analysis of individual items, as follows: i) studies analysing the frequency and severity of individual somatic symptoms; ii) those that investigated gender differences; and iii) studies examining the association between individual items and certain variables such as socioeconomic status and likelihood of suicidal ideation, among others.
The most prevalent symptoms in most of the studies were “pain in your arms, legs, or joints”, “back pain”, “headaches”, and “feeling tired or having low energy”. This finding is consistent with other studies that have assessed somatic symptoms in the general population using different instruments such as the Screening for Somatoform Symptoms (Hiller et al., 2006, Rief et al., 2001, Rief et al., 1997) or the Freiburg Complaint List (Fahrenberg, 1975, Fahrenberg, 1995). Most of those studies also found that different types of pain were among the most prevalent FSS (Hiller et al., 2006, Rief et al., 2001, Fahrenberg, 1975). The high prevalence of headaches and low back pain is not unexpected given that these symptoms are among the most common complaints worldwide in the general population, with a prevalence rate > 25% (Meucci et al., 2015, Stovner et al., 2018).
The findings of the studies in this review that assessed individuals with mental disorders showed that “trouble sleeping”, “feeling tired or having low energy”, “nausea, gas, or indigestion”, “constipation, loose bowels, or diarrhea”, and “stomach pain” were the symptoms most closely associated with emotional disorders (anxiety, depression, and somatoform disorders). These findings are consistent with the results of other studies that have used the PHQ-15 or other similar questionnaires (Lyoo et al., 2014, Bekhuis et al., 2016, Gerber et al., 1992). One study that used the PHQ-15 to screen for depression found that higher scores on the items assessing gastrointestinal symptoms, fatigue, and sleeping problems are good predictors of depression (Lyoo et al., 2014). In fact, gastrointestinal symptoms were a significant predictor of persistent major depressive disorder (MDD) in a study that used the Four-Dimensional Symptom Questionnaire (4DSQ) to assess somatic symptoms (Bekhuis et al., 2016, Gerber et al., 1992), who used the Hopkins Symptom Checklist 49-item depression scale to screen for depression, sleep disorders and fatigue had the highest positive predictive value (61% and 60%, respectively). However, the strong association between low energy and sleeping problems with anxiety and depression might arguably be tautological, as both symptoms are part of the DSM-V diagnostic criteria for anxiety and depression disorders (American Psychiatric Association, 2013). Interestingly, despite the high prevalence of cardiovascular symptoms reported in patients with anxiety and depression (Bekhuis et al., 2016, Tylee and Gandhi, 2005), this association was not evident in the present review, as none of the cardiac-related symptoms such as “chest pain”, “feeling your heart pound or race”, and “fainting spells” were among the most frequently reported in the studies conducted in patients with depression and anxiety (Toussaint et al., 2017, Gonzalez et al., 2009, Grover et al., 2012), nor were they positive correlated with depression or anxiety scales (Carlehed et al., 2017).
Previous studies have shown that somatic symptoms are more common and more intense in women than in men (Barsky et al., 2001, Wool and Barsky, 1994). Kroenke et al. reported marked sex differences in somatic complaints in 13 out of 14 PHQ-15 items (Kroenke and Spitzer, 1998). According to Haug et al., 21 out of 25 somatic symptoms were more common in women than in men (Haug et al., 2004). Our quantitative analysis of gender differences in the PHQ-15 items confirmed that women had a slightly higher overall score. However, we observed a higher prevalence on only 3 items: “headaches” (OR 2.16), “dizziness” (OR 1.58), and “stomach pain” (OR 1.46). However, based on Cohen’s criteria (Cohen, n.d.), the effect size of these differences was small to moderate: 0.42 for “headache”, 0.25 for “dizziness”, and 0.20 for “stomach pain”. The higher prevalence of “headache” and “dizziness” in women is consistent with epidemiological studies showing that headache is two to three times more prevalent in women than men (Vetvik and MacGregor, 2017, Celentano et al., 1990), while dizziness shows a marked female predominance (Bisdorff et al., 2013, Yardley et al., 1998). One of the plausible biological explanations for these gender differences are the effects of gonadal hormones during the reproductive period (Vetvik and MacGregor, 2017), and menopause-associated disorders such as demineralization and metabolic changes (Rask et al., 2016).
Our finding that women scored higher on “stomach pain” is consistent with the higher prevalence of functional disorders such as irritable bowel syndrome (IBS) in women (Kim and Kim, 2018, Chang and Heitkemper, 2002, Sperber et al., 2017). Indeed, a recent review found sex difference in IBS symptoms, which include abdominal pain, dyspepsia, and functional defecatory disorder, with women complaining more frequently of abdominal pain and constipation-related symptoms, while men more commonly report diarrhea-related symptoms (Kim and Kim, 2018). These data may explain this significant gender difference in the item “abdominal pain” and the absence of a difference in other gastrointestinal symptoms such as “constipation, loose bowels, or diarrhea” or “nausea, gas, or indigestion”. Indeed, Rief et al. (2001) found that abdominal pain was more common in women, but mainly in those under the age of 45, probably related to menstrual cramps.
STRENGTHS AND LIMITATIONS
To our knowledge, this is the first systematic review and meta-analysis to examine the outcomes of studies that have analysed the individual PHQ-15 items. An important limitation of this review is related to the scarce number and wide heterogeneity of the studies included in terms of objectives, methodologies, and target population, which precluded us from meta-analyzing all but one of the variables (gender). However, this was somehow offset by a relatively large aggregate sample size. In addition, most of the studies did not stratify the samples by the presence of organic diseases, which could have influenced the prevalence of individual items. Furthermore, the important socioeconomic and cultural differences in the study populations make direct comparisons difficult. The quality assessment (QUADAS-2) showed that most of these studies had an unclear risk of bias since they did not report whether they used the reference standard to verify the index test results (Table S1). However, the risk of applicability concerns was low for all studies. Finally, it should be noted that the search was conducted until November 2019 following the preregistered plan, so more recent papers have not been included. Furthermore, there were excluded doctoral thesis and dissertations, thus we may have missed some unpublished studies with valuable data.
IMPLICATIONS
Despite the wide use of the PHQ-15 in the clinical practice, the prevalence of reported individual item can significantly differ, depending on the group sociodemographic and clinical that potentially can lead to underestimation or overestimation of the total score of the PHQ-15. Our review by reporting those individual items more likely to differ in their prevalence for different sociodemographic and clinical backgrounds, pointed-out the need to conduct further measurement invariance studies in those groups. This will allow clinicians and researchers to more accurately assess whether between-group differences in somatic symptom intensity are true differences and not a measurement artefact. The results of this study upon the frequency and predictive value of different somatic symptoms can favor a more complex and exhaustive assessment of the patient with psychosomatic symptoms. A better understanding of the role of different factors in somatic symptoms can be used both in the diagnostic and treatment processes. The data from the meta-analysis of gender differences may also have important research and clinical implications. For example, it can guide the clinicians to the identification of those patients more prone to present a particular somatic symptom. In this regard, to the best of our knowledge, only one study so far has demonstrated the PHQ-15 to be invariant across both gender and age in a large sample of primary care patients with emotional disorders (Cano-García et al., 2020). Furthermore, given the associations between individual PHQ-15 items and certain sociodemographic characteristics, there is also a need to conduct future studies such as structural equation modelling for testing differential item functioning, which could allow to understand the influence of each individual item on the total score of the PHQ-15.
Future research using the PHQ-15 should prospectively assess the association between different mental disorders and certain FSS patterns, as the cumulative data on these patterns remain scarce. Performing more of these types of studies could increase our understanding of bothersome FSS symptoms, which are often overlooked in routine clinical practice.
Another aspect that merits greater study is the role of gender differences in the individual somatic symptoms. These differences should be investigated in greater depth with close control of potential confounding factors, such as the presence of organic diseases and sociocultural variation. Additionally, there is a notable lack of studies examining the associations between individual items and relevant sociodemographic variable such as age.
CONCLUSIONS
It seems clear that greater use of the PHQ-15 in different clinical settings and non-clinical populations could help to provide a better understanding of somatic symptoms that might otherwise be overlooked. The findings of the present review underscore the associations of specific somatic symptoms, as measured by the PHQ-15, with sociodemographic and clinical variables in different populations. Specifically, our findings provide a better understanding of gender differences in somatic symptoms, and our data suggest that although there are gender differences, overall, these appear to be small in magnitude. Future research should examine the measurement invariance of the scale in different sociodemographic groups.
Declaration of Competing Interest
None.
Acknowledgements
C.G-B was supported by the Valdecilla Biomedical Research Institute (IDIVAL) Grants no. INT/A19/02 and PRIMVAL 18/03.A.P.was supported by the Valdecilla Biomedical Research Institute (IDIVAL) Grant no. PRIMVAL 19/01.
Credit authorship contribution statement
Oleksandr Boiko: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing - original draft. Sara Barrio-Martínez: Data curation, Visualization, Writing - review & editing. Amador Priede: Visualization, Writing - review & editing, Funding acquisition. Ludovica Ventura: Visualization, Writing - review & editing. Nerea Gómez-Carazo: Visualization, Writing - review & editing. Aida Hernández-Abellán: Visualization, Writing - review & editing. Esther Setién-Suero: Visualization, Writing - review & editing. César González-Blanch: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Software, Writing - review & editing.
REFERENCES
American Psychiatric Association, 2013. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association. https://doi.org/10.1176/appi.books.9780890425596
Barsky, A.J., Orav, E.J., Bates, D.W., 2005. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch. Gen. Psychiatry. https://doi.org/10.1001/archpsyc.62.8.903
Barsky, A.J., Peekna, H.M., Borus, J.F., 2001. Somatic symptom reporting in women and men. J. Gen. Intern. Med. 16, 266–26675. https://doi.org/10.1046/j.1525-1497.2001.00229.x
Bekhuis, E., Boschloo, L., Rosmalen, J.G.M., de Boer, M.K., Schoevers, R.A., 2016. The impact of somatic symptoms on the course of major depressive disorder. J. Affect. Disord. 205, 112–118. https://doi.org/10.1016/j.jad.2016.06.030
Bener, A., Al-Kazaz, M., Ftouni, D., Al-Harthy, M., Dafeeah, E.E., 2013. Diagnostic overlap of depressive, anxiety, stress and somatoform disorders in primary care. Asia-Pacific Psychiatry 5. https://doi.org/10.1111/j.1758-5872.2012.00215.x
Beutel, M.E., Wiltink, J., Ghaemi Kerahrodi, J., Tibubos, A.N., Brähler, E., Schulz, A., Wild, P., Münzel, T., Lackner, K., König, J., Pfeiffer, N., Michal, M., Henning, M., 2019. Somatic symptom load in men and women from middle to high age in the Gutenberg Health Study - association with psychosocial and somatic factors. Sci. Rep. https://doi.org/10.1038/s41598-019-40709-0
Bisdorff, A., Bosser, G., Gueguen, R., Perrin, P., 2013. The Epidemiology of Vertigo, Dizziness, and Unsteadiness and Its Links to Co-Morbidities. Front. Neurol. 4. https://doi.org/10.3389/fneur.2013.00029
Borenstein, M., Hedges, L. V, Higgins, J.P.T., Rothstein, H.R., 2013. Comprehensive Meta-Analysis Version 3.
Cano-García, F.J., Muñoz-Navarro, R., Sesé Abad, A., Moretti, L.S., Medrano, L.A., Ruiz-Rodríguez, P., González-Blanch, C., Moriana, J.A., Cano-Vindel, A., 2020. Latent structure and factor invariance of somatic symptoms in the patient health questionnaire (PHQ-15). J. Affect. Disord. 261, 21–29. https://doi.org/10.1016/j.jad.2019.09.077
Carlehed, G., Katz, J., Nordin, S., 2017. Somatic symptoms of anxiety and depression: A population-based study. Ment. Heal. Prev. 6, 57–62. https://doi.org/10.1016/j.mhp.2017.03.005
Carson, A.J., Stone, J., Hansen, C.H., Duncan, R., Cavanagh, J., Matthews, K., Murray, G., Sharpe, M., 2015. Somatic symptom count scores do not identify patients with symptoms unexplained by disease: A prospective cohort study of neurology outpatients. J. Neurol. Neurosurg. Psychiatry 86, 295–301. https://doi.org/10.1136/jnnp-2014-308234
Celentano, D.D., Linet, M.S., Stewart, W.F., 1990. Gender differences in the experience of headache. Soc. Sci. Med. 30, 1289–1295. https://doi.org/10.1016/0277-9536(90)90309-G
Chang, L., Heitkemper, M.M., 2002. Gender differences in irritable bowel syndrome. Gastroenterology 123, 1686–1701. https://doi.org/10.1053/gast.2002.36603
De Waal, M.W.M., Arnold, I.A., Eekhof, J.A.H., Van Hemert, A.M., 2004. Somatoform disorders in general practice: Prevalence, functional impairment and comorbidity with anxiety and depressive disorders. Br. J. Psychiatry 184, 470–476. https://doi.org/10.1192/bjp.184.6.470
Delisle, V.C., Beck, A.T., Dobson, K.S., Dozois, D.J.A., Thombs, B.D., 2012. Revisiting gender differences in somatic symptoms of depression: Much ado about nothing? PLoS One 7, e32490. https://doi.org/10.1371/journal.pone.0032490
Deschepper, R., Six, S., Gidron, Y., Depoorter, A.M., Vandekerckhove, M., Gheysens, N., Van Overmeire, R., Bilsen, J., 2018. Association between feeling threatened by a terrorist attack and subjective health: a web survey a week after the attacks of 22 March 2016 in Belgium. Eur. J. Psychotraumatol. 9. https://doi.org/10.1080/20008198.2018.1500821
Fahrenberg, J., 1995. Somatic complaints in the German population. J. Psychosom. Res. 39, 809–817. https://doi.org/10.1016/0022-3999(94)00151-0
Fahrenberg, J., 1975. The Freiburg Bodily Complaints Inventory (Freiburger Beschwerdenliste [FBL]). [The Freiburg Bodily Complaints Inventory (Freiburger Beschwerdenliste [FBL]).]. Zeitschrift für Klin. Psychol. 4, 79–100.
Fink, P., Hansen, M.S., Oxhøj, M.L., 2004. The prevalence of somatoform disorders among internal medical inpatients. J. Psychosom. Res. 56, 413–418. https://doi.org/10.1016/S0022-3999(03)00624-X
Gerber, P.D., Barrett, J.E., Barrett, J.A., Oxman, T.E., Manheimer, E., Smith, R., Whiting, R.D., 1992. The relationship of presenting physical complaints to depressive symptoms in primary care patients. J. Gen. Intern. Med. 7, 170–173. https://doi.org/10.1007/BF02598007
Gonzalez, D.S., Rodríguez, M., García, C., Prieto, R., Saiz-Ruiz, J., 2009. Gender differences in major depressive disorder: somatic symptoms and quality of life. Rev. Psiquiatr. Salud Ment. 2, 119–27. https://doi.org/10.1016/S1888-9891(09)72402-4
Grover, S., Kumar, V., Chakrabarti, S., Hollikatti, P., Singh, P., Tyagi, S., Kulhara, P., Avasthi, A., 2012. Prevalence and type of functional somatic complaints in patients with first-episode depression. East Asian Arch. Psychiatry.
Haug, T.T., Mykletun, A., Dahl, A.A., 2004. The association between anxiety, depression, and somatic symptoms in a large population: The HUNT-II study. Psychosom. Med. 66, 845–851. https://doi.org/10.1097/01.psy.0000145823.85658.0c
Henningsen, P., Zimmermann, T., Sattel, H., 2003. Medically unexplained physical symptoms, anxiety, and depression: A meta-analytic review. Psychosom. Med. https://doi.org/10.1097/01.PSY.0000075977.90337.E7
Henningsen, P., Zipfel, S., Herzog, W., 2007. Management of functional somatic syndromes. Lancet. https://doi.org/10.1016/S0140-6736(07)60159-7
Hiller, W., Rief, W., Brähler, E., 2006. Somatization in the population: From mild bodily misperceptions to disabling symptoms. Soc. Psychiatry Psychiatr. Epidemiol. 41, 704–712. https://doi.org/10.1007/s00127-006-0082-y
Hinz, A., Ernst, J., Glaesmer, H., Brähler, E., Rauscher, F.G., Petrowski, K., Kocalevent, R.-D., 2017. Frequency of somatic symptoms in the general population: Normative values for the Patient Health Questionnaire-15 (PHQ-15). J. Psychosom. Res. https://doi.org/10.1016/j.jpsychores.2016.12.017
Jeon, H.J., Woo, J.M., Kim, H.J., Fava, M., Mischoulon, D., Cho, S.J., Chang, S.M., Park, D.H., Kim, J.W., Yoo, I., Heo, J.Y., Hong, J.P., 2016. Gender differences in somatic symptoms and current suicidal risk in outpatients with major depressive disorder. Psychiatry Investig. 13, 609–615. https://doi.org/10.4306/pi.2016.13.6.609
Jordan, P., Shedden-Mora, M.C., Löwe, B., 2018. Predicting suicidal ideation in primary care: An approach to identify easily assessable key variables. Gen. Hosp. Psychiatry 51, 106–111. https://doi.org/10.1016/j.genhosppsych.2018.02.002
Kim, Y.S., Kim, N., 2018. Sex-Gender Differences in Irritable Bowel Syndrome. J. Neurogastroenterol. Motil. 24, 544–558. https://doi.org/10.5056/jnm18082
Kocalevent, R.D., Hinz, A., Brähler, E., 2013. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry 13, 91. https://doi.org/10.1186/1471-244X-13-91
Körber, S., Frieser, D., Steinbrecher, N., Hiller, W., 2011. Classification characteristics of the Patient Health Questionnaire-15 for screening somatoform disorders in a primary care setting. J. Psychosom. Res. 71, 142–147. https://doi.org/10.1016/j.jpsychores.2011.01.006
Kroenke, K., Messina III, N., Benattia, I., Graepel, J., Musgnung, J., 2006. Venlafaxine extended release in the short-term treatment of depressed and anxious primary care patients with multisomatoform disorder. J. Clin. Psychiatry. https://doi.org/10.4088/JCP.v67n0111
Kroenke, K., Spitzer, R.L., 1998. Gender differences in the reporting of physical and somatoform symptoms. Psychosom. Med. 60, 150–155. https://doi.org/10.1097/00006842-199803000-00006
Kroenke, K., Spitzer, R.L., Williams, J.B.W., Löwe, B., 2010. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry. https://doi.org/10.1016/j.genhosppsych.2010.03.006
Leonhart, R., Tang, L., Pang, Y., Li, J., Song, L., Fischer, I., Koch, M., Wuensch, A., Fritzsche, K., Schaefert, R., 2017. Physical and psychological correlates of high somatic symptom severity in Chinese breast cancer patients. Psychooncology. 26, 656–663. https://doi.org/10.1002/pon.4203
Liberati, A., Altman, D.G., Tetzlaff, J., Mulrow, C., Gøtzsche, P.C., Ioannidis, J.P.A., Clarke, M., Devereaux, P.J., Kleijnen, J., Moher, D., 2009. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 6, e1000100. https://doi.org/10.1371/journal.pmed.1000100
Lyoo, Y.C., Ju, S., Kim, E., Kim, J.E., Lee, J.H., 2014. The patient health questionnaire-15 and its abbreviated version as screening tools for depression in Korean college and graduate students. Compr. Psychiatry 55, 743–748. https://doi.org/10.1016/j.comppsych.2013.11.011
Madan, A., Clapp, J., Osborne, P., Walker, C., Frueh, B.C., Allen, J., Oldham, J., Fowler, J.C., 2016. Improvements in somatic complaints among individuals with serious mental illness receiving treatment in a psychiatric hospital. Psychosom. Med. https://doi.org/10.1097/PSY.0000000000000298
Marks, E.M., Hunter, M.S., 2015. Medically Unexplained Symptoms: An acceptable term? Br. J. Pain. https://doi.org/10.1177/2049463714535372
Mejía-Rodríguez, D., Rodríguez, R., Restrepo, D., 2019. Sociodemographic Characterization and Psychiatric Symptoms of Patients With Medically Unexplained Symptoms in a Healthcare Institution in Medellin (Colombia). Rev. Colomb. Psiquiatr. 48, 72–79. https://doi.org/10.1016/j.rcp.2017.08.005
Meucci, R.D., Fassa, A.G., Xavier Faria, N.M., 2015. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica. https://doi.org/10.1590/S0034-8910.2015049005874
Morawa, E., Dragano, N., Jöckel, K.H., Moebus, S., Brand, T., Erim, Y., 2017. Somatization among persons with Turkish origin: Results of the pretest of the German National Cohort Study. J. Psychosom. Res. 96, 1–9. https://doi.org/10.1016/j.jpsychores.2017.02.014
Rask, M.T., Carlsen, A.H., Budtz-Lilly, A., Rosendal, M., 2016. Multiple somatic symptoms in primary care patients: a cross-sectional study of consultation content, clinical management strategy and burden of encounter. BMC Fam. Pract. 17, 100. https://doi.org/10.1186/s12875-016-0478-z
Rief, W., Hessel, A., Braehler, E., 2001. Somatization symptoms and hypochondriacal features in the general population. Psychosom. Med. 63, 595–602. https://doi.org/10.1097/00006842-200107000-00012
Rief, W., Hiller, W., Heuser, J., 1997. SOMS: das Screening für somatoforme Störungen; Manual zum Fragebogen; mit zusätzlichen Informationen zur Hypochondrie-Messung und zum Einsatz von.
Roca, M., Gili, M., Garcia-Garcia, M., Salva, J., Vives, M., Garcia Campayo, J., Comas, A., 2009. Prevalence and comorbidity of common mental disorders in primary care. J. Affect. Disord. 119, 52–58. https://doi.org/10.1016/j.jad.2009.03.014
Shidhaye, R., Mendenhall, E., Sumathipala, K., Sumathipala, A., Patel, V., 2013. Association of somatoform disorders with anxiety and depression in women in low and middle income countries: A systematic review. Int. Rev. Psychiatry. https://doi.org/10.3109/09540261.2012.748651
Sitnikova, K., Dijkstra-Kersten, S.M.A., Mokkink, L.B., Terluin, B., van Marwijk, H.W.J., Leone, S.S., van der Horst, H.E., van der Wouden, J.C., 2017. Systematic review of measurement properties of questionnaires measuring somatization in primary care patients. J. Psychosom. Res. https://doi.org/10.1016/j.jpsychores.2017.10.005
Sperber, A.D., Dumitrascu, D., Fukudo, S., Gerson, C., Ghoshal, U.C., Gwee, K.A., Hungin, A.P.S., Kang, J.Y., Minhu, C., Schmulson, M., Bolotin, A., Friger, M., Freud, T., Whitehead, W., 2017. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 66, 1075–1082. https://doi.org/10.1136/gutjnl-2015-311240
Spitzer, R.L., Kroenke, K., Williams, J.B.W., 1999. Validation and utility of a self-report version of PRIME-MD: The PHQ Primary Care Study. J. Am. Med. Assoc. 282, 1737–1744. https://doi.org/10.1001/jama.282.18.1737
Stovner, L.J., Nichols, E., Steiner, T.J., Abd-Allah, F., Abdelalim, A., Al-Raddadi, R.M., Ansha, M.G., Barac, A., Bensenor, I.M., Doan, L.P., Edessa, D., Endres, M., Foreman, K.J., Gankpe, F.G., Gopalkrishna, G., Goulart, A.C., Gupta, R., Hankey, G.J., Hay, S.I., Hegazy, M.I., Hilawe, E.H., Kasaeian, A., Kassa, D.H., Khalil, I., Khang, Y.H., Khubchandani, J., Kim, Y.J., Kokubo, Y., Mohammed, M.A., Moradi-Lakeh, M., Nguyen, H.L.T., Nirayo, Y.L., Qorbani, M., Ranta, A., Roba, K.T., Safiri, S., Santos, I.S., Satpathy, M., Sawhney, M., Shiferaw, M.S., Shiue, I., Smith, M., Szoeke, C.E.I., Truong, N.T., Venketasubramanian, N., Weldegwergs, K.G., Westerman, R., Wijeratne, T., Tran, B.X., Yonemoto, N., Feigin, V.L., Vos, T., Murray, C.J.L., 2018. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 17, 954–976. https://doi.org/10.1016/S1474-4422(18)30322-3
Toft, T., Fink, P., Oernboel, E., Christensen, K., Frostholm, L., Olesen, F., 2005. Mental disorders in primary care: Prevalence and co-morbidity among disorders. Results from the Functional Illness in Primary care (FIP) study. Psychol. Med. 35, 1175–1184. https://doi.org/10.1017/S0033291705004459
Toussaint, A., Kroenke, K., Baye, F., Lourens, S., 2017. Comparing the Patient Health Questionnaire – 15 and the Somatic Symptom Scale – 8 as measures of somatic symptom burden. J. Psychosom. Res. https://doi.org/10.1016/j.jpsychores.2017.08.002
Tylee, A., Gandhi, P., 2005. The importance of somatic symptoms in depression in primary care. Prim. Care Companion J. Clin. Psychiatry. https://doi.org/10.4088/PCC.v07n0405
Vetvik, K.G., MacGregor, E.A., 2017. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. https://doi.org/10.1016/S1474-4422(16)30293-9
Whiting, P.F., Rutjes, A.W.S., Westwood, M.E., Mallett, S., Deeks, J.J., Reitsma, J.B., Leeflang, M.M.G., Sterne, J.A.C., Bossuyt, P.M.M., 2011. Quadas-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. https://doi.org/10.7326/0003-4819-155-8-201110180-00009
Wilkie, S., Crawley, R., Button, S., Thornton, A., Ayers, S., 2018. Assessing physical symptoms during the postpartum period: reliability and validity of the primary health questionnaire somatic symptom subscale (PHQ-15). J. Psychosom. Obstet. Gynecol. 39, 56–63. https://doi.org/10.1080/0167482X.2017.1289167
Witthöft, M., Hiller, W., Loch, N., Jasper, F., 2013. The latent structure of medically unexplained symptoms and its relation to functional somatic syndromes. Int. J. Behav. Med. 20, 172–183. https://doi.org/10.1007/s12529-012-9237-2
Wolfe, F., Walitt, B.T., Katz, R.S., Häuser, W., 2014. Symptoms, the nature of fibromyalgia, and diagnostic and statistical manual 5 (DSM-5) defined mental illness in patients with rheumatoid arthritis and fibromyalgia. PLoS One 9, e88740. https://doi.org/10.1371/journal.pone.0088740
Wool, C.A., Barsky, A.J., 1994. Do Women Somatize More Than Men? Gender Differences in Somatization. Psychosomatics. https://doi.org/10.1016/S0033-3182(94)71738-2
Yardley, L., Owen, N., Nazareth, I., Luxon, L., 1998. Prevalence and presentation of dizziness in a general practice community sample of working age people. Br. J. Gen. Pract. 48, 1131–1135.
Zhang, Xinyao, Zhang, Xiaoye, 2017. Somatization symptoms in lung cancer patients and correlative analysis between anxiety, depression and somatization symptoms. Chinese J. Lung Cancer 20, 473–478. https://doi.org/10.3779/j.issn.1009-3419.2017.07.06
Zijlema, W.L., Stolk, R.P., Löwe, B., Rief, W., White, P.D., Rosmalen, J.G.M., 2013. How to assess common somatic symptoms in large-scale studies: A systematic review of questionnaires. J. Psychosom. Res. https://doi.org/10.1016/j.jpsychores.2013.03.093