Original
Emotional intelligence abilities of caregivers of patients with acquired brain injury and cognitive impairment: are they related to overload or resilience?
Irene de-Torres García (a,b, Fernando Bustos (b,d, Juan Carlos Arango-Lasprilla (c, Pablo Fernández-Berrocal (b
- Málaga Regional University Hospital, Málaga, Spain
- Department of Basic Psychology, Faculty of Psychology, University of Málaga, Málaga, Spain.
- Biocruces Bizkaia Health Research Institute, IKERBASQUE, Basque Foundation for Science, Barakaldo, Bizkaia, Spain
- Department of Language and Linguistics, University of Essex.
Ansiedad y Estrés, 28, (2022), 55-61
https://doi.org/10.5093/anyes2022a6
https://www.ansiedadyestres.es
Bibliography reference
INFO ARTICLE
Recibido el 21 de diciembre de 2021
Aceptado el 1 de agosto de 2021
Online el 24 de 12 de 2021
ABSTRACT
Introduction: Acquired brain injury entails stressful situations of emotional complexity. Objective: To evaluate possible relationship among emotional intelligence, emotional status, resilience, and burden sensation of caregivers of patients with cognitive-behavioral impairment due to acquired brain injury in isolation circumstances because of COVID-19 pandemic.
Material and methods: An observational descriptive cross-sectional study of prevalence was designed with a sample of 17 caregivers of patients with cognitive-behavioral impairment due to acquired brain injury. Main outcome measures: Caregiver Burden Interview, the 10-item Connor-Davidson Resilience Scale, Emotional Health, the Trait Meta-Mood Scale and the Positive and Negative Affect Schedule.
Results: The median age of the 17 caregivers was 47.5 years, 71% of women had a median care-time of 3.5 years, and 65% of the total sample were spouses of the patients. 70% of the patients were affected by stroke (hemorrhagic or ischemic cause). 59% of the caregivers presented a low level of emotional attention and emotional clarity, and 47 %, low emotional repair ability. 82% of them did not report overload, 53% showed low resilience level. Emotional intelligence showed strong correlation with resilience and mental health of caregivers. All of them were positively correlated with daily positive emotions and negatively correlated with negative emotions and overload.
Conclusions: Emotional intelligence, resilience, and mental health of caregivers are strongly correlated. All of them increase positive emotions and reduce negative emotions and overload.
KEYWORDS
Emotional intelligence
Caregiver
Brain injury
Cognitive impairment
Resilience
Overload
Inteligencia emocional en cuidadores de pacientes con daño cerebral adquirido y déficit cognitivo: ¿existe relación con la sobrecarga o la resiliencia?
Ansiedad y Estrés, 28, (2022), 55-61
https://doi.org/10.5093/anyes2022a6
https://www.ansiedadyestres.es
Bibliography reference
RESUMEN
Introducción: el daño cerebral adquirido crea situaciones estresantes y de gran complejidad emocional. Objetivo: evaluar relación entre inteligencia emocional, resiliencia, estado emocional y sobrecarga de los cuidadores de pacientes con daño cerebral adquirido y afectación cognitivo-conductual en circunstancias de aislamiento por pandemia COVID-19.
Materiales y métodos: estudio observacional descriptivo transversal de prevalencia. Participantes: 17 cuidadores de pacientes con daño cerebral adquirido y afectación cognitivo- conductual. Principales medidas: Cuestionario sobre Carga del Cuidador, Medida de Resiliencia Connor- Davidson, Cuestionario de Salud Emocional, Escala Trait Meta-Mood y Escala de Afecto Positivo y Negativo.
Resultados: mediana de edad 47,5 años, 71% mujeres, mediana de tiempo siendo cuidador 3,5 años y 65% de la muestra eran cónyuges. El 70% de los pacientes habían sufrido un ictus y el principal deterioro cognitivo de ellos, referido por familiares, fue el déficit de memoria. El 59% de los cuidadores presentó bajo nivel de atención emocional y claridad emocional, y el 47%, baja capacidad de reparación emocional. El 82% no informó sobrecarga, el 53% mostró un bajo nivel de resiliencia y un afecto positivo en el mes previo ligeramente más alto que el afecto negativo. La inteligencia emocional mostró una fuerte correlación con la resiliencia y la salud mental. Además, estas tres variables correlacionaron positivamente con las emociones positivas y negativamente con las negativas y la sobrecarga.
Conclusiones: Inteligencia emocional, resiliencia y salud mental están fuertemente correlacionadas. Las tres aumentan las emociones positivas y reducen las negativas y la sobrecarga. La sobrecarga asocia peor resiliencia, reparación emocional y salud mental.
PALABRAS CLAVE
Cuidador
Inteligencia emocional
Daño cerebral
Déficit cognitivo
Resiliencia
Sobrecarga
INTRODUCTION
An acquired brain injury (ABI) is a complex medical situation often followed by a broad range of physical, cognitive, emotional, and behavioral disturbances (Hoeffding et al., 2017). ABI can be caused by traumatic brain injury (TBI) or stroke (hemorrhagic or ischemic), among others. It brings stressful situations of great emotional complexity for the patient and their relatives. For this reason, this study is specially focused on the overload suffered by caregivers of patients with ABI and cognitive impairment. ABI research revealed that brain damaged patients may present cognitive impairment which entails multiple behavioral disturbances, such as having difficulties reading social cues from others and being viewed as self-centered and unresponsive to the caregiver's needs (Riley, 2016). Changes in the patient's personality and behavior can create in the partner a perception that the injured person's identity has undergone a total transformation. In addition, the partner may be required to manage relationships between the patient and other relatives. In the case of injured children, ABI poses additional concerns regarding a long-term impact on the family or the probability of neglecting their children's needs. Some caregivers may even restrict social contact to avoid uncomfortable situations (Riley, 2016). Authors as Liu et al. (2019) highlighted stressors for caregivers of patients with cognitive impairment, in that case due to dementia. They described from the point of view of the stress process model, the differentiation between primary and secondary stressors. Primary stressors are directly related to caregiving, such as behavioral changes, cognitive status, and level of dependency of the patient. Secondary stressors are the consequences of changes caused by the role, including work-family conflict and financial stress.
There is a bidirectional relationship between the wellbeing of the family and the patient (Hoeffding et al., 2017). For example, the latter may depend on another person for daily planning; hence, decision making becomes a collaborative work with the caregiver. It can be useful and comforting in this process the fact of understanding the functional implications of the ABI on the patient; this information has to proceed from medical institutions to facilitate the resilient transformation of all the members affected (Knox et al., 2015). Families need develop progressively adaptive capacities to establish effective psychosocial coping while living with patients with behavioral problems (Karpa et al., 2020). These adaptive capacities are related to emotional intelligence (EI) tools, in fact, EI refers to the ability to identify, express and understand emotions, assimilate, and regulate them in oneself and others (Salovey & Mayer, 1990). The most emotionally intelligent individuals will have better mental health, which will consequently affect the mental health of their family (Sánchez et al., 2006). Emotional regulation is the ability to influence our emotions, about when we have them, about how we experience and express them. Co-regulation occurs when the caregiver helps their relative to regulate emotions. Thus, EI abilities help caregivers cope with patients' behavioral disturbances and their own negative emotions in reaction to these changes.
In the counterpart, the caregiving experience often alters the physical and psychological health of the caregivers (Gebhardt et al., 2011). Their anxiety is often managed through overprotective practices that put them at risk of burnout (Lond & Williamson, 2018). The current situation related to the COVID-19 pandemic worsens caregivers' situation because of quarantine measures as a disease control tool (Dubey et al., 2020). Isolation and lack of routines turn more challenging the care of a patient with cognitive impairment.
The main objective of the present study is to evaluate possible relationship among EI, resilience, emotional status, and burden sensation of caregivers of patients with cognitive- behavioral impairment due to ABI in isolation circumstances because of the COVID-19 pandemic.
It is considered a secondary objective of this research to assess deficits of EI or resilience with the focus in the design of psychological interventions for caregivers to help them to cope with the situation.
INTRODUCTION
An acquired brain injury (ABI) is a complex medical situation often followed by a broad range of physical, cognitive, emotional, and behavioral disturbances (Hoeffding et al., 2017). ABI can be caused by traumatic brain injury (TBI) or stroke (hemorrhagic or ischemic), among others. It brings stressful situations of great emotional complexity for the patient and their relatives. For this reason, this study is specially focused on the overload suffered by caregivers of patients with ABI and cognitive impairment. ABI research revealed that brain damaged patients may present cognitive impairment which entails multiple behavioral disturbances, such as having difficulties reading social cues from others and being viewed as self-centered and unresponsive to the caregiver's needs (Riley, 2016). Changes in the patient's personality and behavior can create in the partner a perception that the injured person's identity has undergone a total transformation. In addition, the partner may be required to manage relationships between the patient and other relatives. In the case of injured children, ABI poses additional concerns regarding a long-term impact on the family or the probability of neglecting their children's needs. Some caregivers may even restrict social contact to avoid uncomfortable situations (Riley, 2016). Authors as Liu et al. (2019) highlighted stressors for caregivers of patients with cognitive impairment, in that case due to dementia. They described from the point of view of the stress process model, the differentiation between primary and secondary stressors. Primary stressors are directly related to caregiving, such as behavioral changes, cognitive status, and level of dependency of the patient. Secondary stressors are the consequences of changes caused by the role, including work-family conflict and financial stress.
There is a bidirectional relationship between the wellbeing of the family and the patient (Hoeffding et al., 2017). For example, the latter may depend on another person for daily planning; hence, decision making becomes a collaborative work with the caregiver. It can be useful and comforting in this process the fact of understanding the functional implications of the ABI on the patient; this information has to proceed from medical institutions to facilitate the resilient transformation of all the members affected (Knox et al., 2015). Families need develop progressively adaptive capacities to establish effective psychosocial coping while living with patients with behavioral problems (Karpa et al., 2020). These adaptive capacities are related to emotional intelligence (EI) tools, in fact, EI refers to the ability to identify, express and understand emotions, assimilate, and regulate them in oneself and others (Salovey & Mayer, 1990). The most emotionally intelligent individuals will have better mental health, which will consequently affect the mental health of their family (Sánchez et al., 2006). Emotional regulation is the ability to influence our emotions, about when we have them, about how we experience and express them. Co-regulation occurs when the caregiver helps their relative to regulate emotions. Thus, EI abilities help caregivers cope with patients' behavioral disturbances and their own negative emotions in reaction to these changes.
In the counterpart, the caregiving experience often alters the physical and psychological health of the caregivers (Gebhardt et al., 2011). Their anxiety is often managed through overprotective practices that put them at risk of burnout (Lond & Williamson, 2018). The current situation related to the COVID-19 pandemic worsens caregivers' situation because of quarantine measures as a disease control tool (Dubey et al., 2020). Isolation and lack of routines turn more challenging the care of a patient with cognitive impairment.
The main objective of the present study is to evaluate possible relationship among EI, resilience, emotional status, and burden sensation of caregivers of patients with cognitive- behavioral impairment due to ABI in isolation circumstances because of the COVID-19 pandemic.
It is considered a secondary objective of this research to assess deficits of EI or resilience with the focus in the design of psychological interventions for caregivers to help them to cope with the situation.
METHODS
An observational descriptive cross-sectional study of prevalence was designed. Two ways were used to contact by e-mail with caregivers of brain injury patients with cognitive impairment: (a) those who were attended in the Cognitive Rehabilitation Clinic in the Regional University Hospital of Málaga and (b) through contact with the brain injury association of our city, ADACEMA (Málaga Brain Injury Association). 17 of the contacted caregivers accepted to enroll in the study during period under COVID-19 mandatory self-isolation order. Hence, 17 caregivers of patients with cognitive-behavioral impairment due to ABI were emotionally evaluated. Inclusion criteria were adult caregivers of an adult patient with cognitive impairment after ABI. Exclusion criteria were non-cognitive impairment of the patient (to avoid bias because of influence in caregivers' burden) and/or age under 18 years old.
Through a web-link, to get a complete description of the sample, caregivers were asked to answer questions about age, gender, number of years as a caregiver, relationship with the patient, presence of more dependent people in their charge, cause of brain injury of the patient, main cognitive deficit of the patient from the point of view of the caregiver. Moreover, several tests were administered: Caregiver Burden Interview (Zarit's Questionnaire; Zarit et al., 1980), the 10-item Connor-Davidson Resilience Scale (10-item CD-RISC; Notario-Pacheco et al., 2011), Emotional Health (MH5; Alonso et al., 1995), the Trait Meta-Mood Scale (TMMS-24; Fernández-Berrocal et al., 2004) and the Positive and Negative Affect Schedule (PANAS; Díaz-García et al., 2020).
Zarit's Questionnaire evaluates factors contributing to feelings Resultados: mediana de edad 47,5 años, 71% mujeres, mediana de tiempo siendo cuidador 3,5 años y 65% de la muestra eran cónyuges. El 70% de los pacientes habían sufrido un ictus y el principal deterioro cognitivo de ellos, referido por familiares, fue el déficit de memoria. El 59% de los cuidadores presentó bajo nivel de atención emocional y claridad emocional, y el 47%, baja capacidad de reparación emocional. El 82% no informó sobrecarga, el 53% mostró un bajo nivel de resiliencia y un afecto positivo en el mes previo ligeramente más alto que el afecto negativo. La inteligencia emocional mostró una fuerte correlación con la resiliencia y la salud mental. Además, estas tres variables correlacionaron positivamente con las emociones positivas y negativamente con las negativas y la sobrecarga. Conclusiones: Inteligencia emocional, resiliencia y salud mental están fuertemente correlacionadas. LAs tres aumentan las emociones positivas y reducen las negativas y la sobrecarga. La sobrecarga asocia peor resiliencia, reparación emocional y salud mental. I. de-Torres García et al. / Ansiedad y Estrés 28(1) (2022) 55-61 57 of the burden of caregivers of patients. The range of score is 0-88, less than 46 points corresponds to an absence of overload, 46–56 shows overload and more than 56, intense overload (Zarit et al., 1980). Yu et al. (2019) showed an optimal cut-off score of 48 to distinguish lower and higher burden for risk of psychological distress, with sensitivity of 73% and specificity of 80% for depression. The Zarit's Questionnaire is the most widely used tool for measuring the level of subjective burden among caregivers, it has been validated across many populations of caregivers (Yu et al., 2019). The 10-item CD-RISC (Notario-Pacheco et al., 2011) is an instrument for measuring resilience that has shown significant psychometric properties. Resilience has been defined as a dynamic process of adaptation to changes in life circumstances. The user has to answer the level of agreement to ten sentences about the previous month. The range of punctuation of this test is 0–40. Equal or less than 27 points is considered low resilience, 28–35 show an adequate level and 36 or more, a high resilient capacity (Notario-Pacheco et al., 2011). 10-item CD-RISC measures are very highly correlated with scores on the original 25-item CD-RISC (r = .92; Campbell-Sills, 2007).
MH5 is part of the Short Form-36 Health Survey (Alonso et al., 1995). It is one of the most widely used and evaluated generic health-related quality of life questionnaires. MH5 is composed of 5 questions about mental health to which the user has to answer about the frequency of the experience of some feelings in the previous four weeks. The range of punctuation is 1–6; being 6 the maximum emotional health quality index (Alonso et al., 1995). Short Form-36 Health Survey has shown high internal consistency (LoMartire et al., 2020).
The TMMS-24 (Fernández-Berrocal et al., 2004) was designed to assess relatively stable individual differences in people's tendency to attend to their moods and emotions, to discriminate clearly and regulate them. Results are divided into three dimensions: attention (I am able to feel and express feelings appropriately), clarity (I understand my emotional states well), and repair (I am able to regulate emotional states correctly). Scores are adapted to men and women population. Each one of the three key dimensions (attention to feelings, emotional clarity, and repair and regulation of the emotions) are evaluated on a five-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). Fernández-Berrocal et al. (2004) obtained alphas of .90, .90, and .86, respectively.
The Positive and Negative Affect Schedule (PANAS; Díaz-García et al., 2020), which is one of the most used affect measures, is a 20-item self-report questionnaire. The range of punctuation is 10–50 for positive affect as well as for negative affect; being 10 the less presence of positive/negative affect in life of the user in the previous month, and 50 the maximum. Díaz- García et al. (2020) showed statistically significant pretest-posttest differences for both PANAS-Positive and PANAS-Negative, with moderate to large effect sizes, suggesting that the scale is able to detect changes in affectivity and, therefore, can be used to examine the impact of an intervention.
Statistical Analysis
Non-parametric descriptive measures and tests are applied. In order to look for relationship among variables with statistical significance, Kruskal Wallis and Mann-Whitney are employed. Normal distribution is studied through the one-sample Kolmogorov-Smirnov Normal Test in order to calculate correlations among variables. Statistical significance is considered at p < .05. SPSS-26 is the statistical software used as a facilitator.
RESULTS
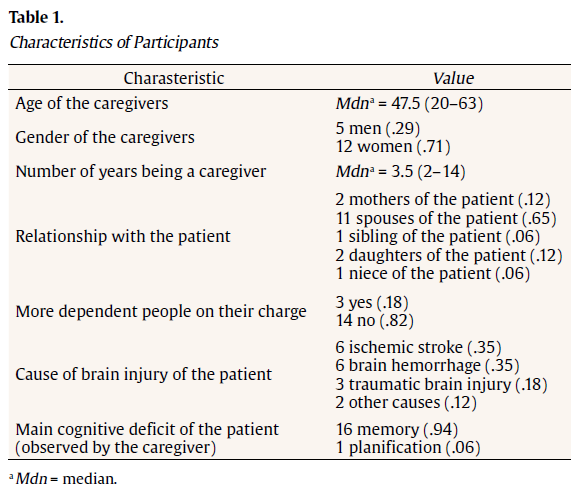
Table 1 presents the sample's characteristics. The median age of the 17 caregivers was 47.5 years old, 71% of women had a median care-time of 3.5 years. 65% of them were spouses of the patients, and 70% of the patients were affected by stroke (hemorrhagic or ischemic cause). The main cognitive impairment of the patients reported by relatives was memory deficit (94%).
Table - 1
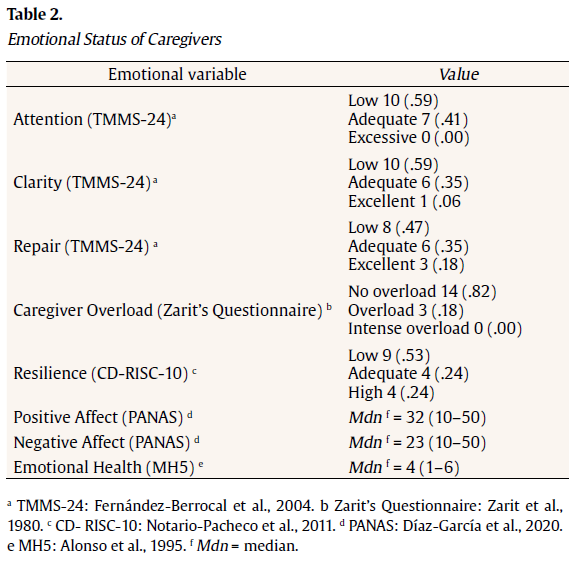
The emotional status of caregivers is described in Table 2. The total of the scale-scores were available for all the participants of this study.
Table - 2
A predominance of low levels compared to general population can be seen in the following results: 59% of them presented a low level of emotional attention and emotional clarity in comparison with global population according to scale's references; 47% of them reported a low ability to repair their emotions compared to general population (TMMS-24; Fernández- Berrocal et al., 2004); and 53% showed low resilience level (10-item CD-RISC; Notario- Pacheco et al., 2011).
Table - 3
Closer results to general population were seen according to 82% of the caregivers did not report overload (Zarit's Questionnaire; Zarit et al., 1980), positive affect was slightly higher than negative in the previous month (Mdn = 32 vs. 23; PANAS; Díaz-García et al., 2020) and the median emotional health quality was 4 (1–6 range; MH5; Alonso et al., 1995).
Figure - 1
Table - 4
Statistically Significant Relationships among Variables
Kruskal Wallis test showed relationship among positive emotions (PANAS; Díaz-García et al., 2020) and the following variables: resilience (p = 0.012; CD-RISC-10; Notario-Pacheco et al., 2011); emotional clarity (p = .023; TMMS-24: Fernández-Berrocal et al., 2004; Figure 1); emotional repair (p = .004; TMMS-24: Fernández- Berrocal et al., 2004; Figure 1). Mann- Whitney test was used to I. de-Torres García et al. / Ansiedad y Estrés 28(1) (2022) 55-61 59 reveal relationship between positive emotions (PANAS; Díaz-García et al., 2020) and gender (p = .037; women associated more positive emotions than men the previous month).
Emotional clarity was related to emotional attention (p = .040; Kruskal Wallis) and emotional repair (p = .004; Kruskal Wallis; TMMS-24: Fernández-Berrocal et al., 2004).
Emotional repair also was related to emotional attention (p = .027; Kruskal Wallis) and resilience (p = .010; Kruskal Wallis; CDRISC- 10: Notario-Pacheco). These statistical relationships are shown in Table 3.
Kruskal Wallis test showed relationship among positive emotions (PANAS; Díaz-García et al., 2020) and the following variables: emotional clarity (p = .023; TMMS-24: Fernández-Berrocal et al., 2004) and emotional repair (p = .004; TMMS-24: Fernández-Berrocal et al., 2004).
DISCUSSION
The objective of this study was to evaluate possible relationship among EI, resilience, emotional status, and burden sensation of caregivers of patients with cognitive-behavioral impairment due to ABI in isolation circumstances because of the COVID-19 pandemic. A predominance of low levels compared to general population were found in our sample related to emotional attention; emotional clarity; ability to repair their emotions (TMMS-24; Fernández-Berrocal et al., 2004); and resilience level (10-item CD-RISC; Notario- Pacheco et al., 2011). Closer results to general population were seen according to absence of overload (Zarit's Questionnaire; Zarit et al., 1980), slight predominance of positive affect versus negative (PANAS; Díaz-García et al., 2020), and preserved emotional health quality (MH5; Alonso et al., 1995).
A low level of emotional attention in TMMS-24 (Fernández-Berrocal et al., 2004) could provoke that caregivers do not take care of their emotional wellbeing. Paying attention to one's emotional status is considered to be the starting point towards a better understanding and reparation of emotions. Furthermore, an adequate level of emotional understanding will increase emphatic abilities. Overall, the caregivers of our sample answered with a low agreement to TMMS-24 items as in "I often think about my feelings" or "I pay close attention to how I feel" (Fernández-Berrocal et al., 2004). Our participants scored better in emotional repair than in attention and clarity. It could be argued that if they dedicated more energy to attend and understand emotions at an earlier stage, reparation could not be as necessary for them daily. Emotional regulation abilities are helpful to balance the mood, but at the same time they are energy-demanding; therefore, an earlier response using attention and clarity abilities would be an excellent strategy to reduce emotional and cognitive overload.
In our study sample, positive emotions (active, energetic, decided, proud, etc.) experienced for caregivers in the previous month were positively related to their levels of resilience and EI (clarity and repair). So, those with better EI and resilient abilities experienced more positive emotions in their daily life, fact that can stimulate motivation and cognition (Scheweder & Raufelder, 2019), even positive emotions may broaden social resources and lead to positive outcomes over time (Fredrickson, 2001).
Women presented a bigger tendency to experience positive emotions than men, but it has to be considered that gender and age is not balanced in our sample, so this tendency should be confirmed. In contrast, Cornelius-White (2007) and Scheweder and Raufelder (2019) defend that there are no gender-related differences in the performance of positive emotions.
In the present study, EI areas were related among them as well: caregivers with better results in emotional clarity associated higher levels of emotional attention and repair, or those with more repair ability associated better emotional attention. EI was also linked to resilience, specially through emotional repair. Other authors have related EI and resilience before (Kong et al., 2016).
Resilience is an active process that involves a set of mechanisms leading to avoid some of the negative consequences of extreme stress in individuals. Six primary psychosocial resilience factors have been described: (a) positive emotions and optimism, (b) cognitive flexibility, (c) religion and spirituality, (d) life meaning, (e) social support and (f) active coping style (Faye et al., 2018). It is important to highlight that in our sample, even with a generalized low level of resilient thoughts, emotional attention, clarity and repair, the majority of the caregivers did not report overload. However, one of the Zarit's Questionnaire (Zarit et al., 1980) sentences in which there was a general agreement among participants was "I feel that my relative depends on me". Even with a general low level of overload (Zarit's Questionnaire: Zarit et al., 1980) in the sample, it showed positively correlation with negative emotions (PANAS: Díaz-García et al., 2020) so more overload caregivers reported, more daily negative emotions they presented. Overload (Zarit's Questionnaire: Zarit et al., 1980) was negatively correlated with EI (TMMS- 24: Fernández-Berrocal et al., 2004), mental health (MH5: Alonso et al., 1995), resilience (CD- RISC-10: Notario-Pacheco et al., 2011) and positive emotions (PANAS: Díaz-García et al., 2020). Interestingly, negative emotions (PANAS: Díaz-García et al., 2020) correlation analysis showed negatively relationship with resilience (CDRISC- 10: Notario-Pacheco et al., 2011), emotional repair (TMMS-24: Fernández-Berrocal et al., 2004) and mental health (MH5: Alonso et al., 1995), but positively relationship to positive emotions (PANAS: Díaz-García et al., 2020), emotional attention, clarity (TMMS-24: Fernández-Berrocal et al., 2004) and overload (Zarit's Questionnaire: Zarit et al., 1980). An explanation for the last point could be that more emotional attention and clarity could help caregivers to realize and attend their own emotions even they are negative or positive, so they can reflex it when responding to the PANAS questionnaire (PANAS: Díaz-García et al., 2020).
Long-lasting caring for a partner with ABI presents considerable challenges that may threaten a person's well-being (Lond & Williamson, 2018). The caregiver often plays a significant role in providing the injured person with emotional support. For many relatives, dealing with these extra demands means that they have little time left to address their own needs (Riley, 2016).
Some consequences of the COVID-19 pandemic are the reduction of social and sanitary support for patients with chronic diseases, with the consequent reduction or cessation of rehabilitation therapies or daycare center activities. This type of patient is sensitive to change in routines, and caregivers will suffer an extra effort to ensure that the patient follows the COVID-19 transmission and protective measures. Even our sample is not large, the need for an EI training for caregivers in isolation circumstances was found in them, so a synchronous online training program on EI was designed. The intervention program would consist of four sessions of three hours of duration. The following topics would be addressed: (a) perception and expression of emotions; (b) assimilation of emotion into thought; (c) emotional understanding; and (d) reflective regulation of emotions. Dynamic interventions would be used to promote group participation and interaction through experiential and reflective activities. Each week, collaborative discussion about previous concepts would be facilitated to connect them to emotional tools and coping strategies. Examples of daily life would be used to promote the understanding of key messages.
The hypothesis is that an EI program would increase caregivers' abilities to attend, understand and repair emotions (their and patients' emotions) to improve their resilient thoughts and increase the frequency of pleasant emotions versus negative ones daily. This hypothesis is based in the results of this study: emotional attention, clarity (TMMS-24: Fernández-Berrocal et al., 2004), and positive emotions (PANAS: Díaz-García et al., 2020) were positively correlated with emotional repair (TMMS-24: Fernández-Berrocal et al., 2004), mental health (MH5: Alonso et al., 1995), and resilience (CD-RISC-10: Notario-Pacheco et al., 2011); in addition, emotional repair (TMMS-24: Fernández-Berrocal et al., 2004), mental health (MH5: Alonso et al., 1995), and resilience (CD-RISC-10: Notario-Pacheco et al., 2011) were negatively correlated with negative emotions (PANAS: Díaz-García et al., 2020) and overload (Zarit's Questionnaire: Zarit et al., 1980), and positively correlated with positive emotions (PANAS: Díaz- García et al., 2020), emotional attention, and clarity (TMMS-24: Fernández- Berrocal et al., 2004).
Besides, this type of intervention may permit a meeting with other caregivers in similar circumstances what could be very valued in a context in which caregivers frequently ask for more support networks. Bryony and Sharman (2015) defend that barriers such as the lack of understanding about the changes involved with ABI could all be minimized with appropriate education about the effects of ABI and specialized counselling services: skills workshops, coping strategies to deal with the behavioral disturbances. It has been defended that routine assessment of resilience might be beneficial to the rehabilitation team in understanding patients and their families (Rapport et al., 2020). Given the long-term challenges of ABI, there is increasing recognition for the need to develop a resilience-building approach to patients and their relatives (Kreutzer et al., 2018). Researchers identified strategies for increasing resilience in persons with TBI and couples: focus on strengthening experiences, integrate supportive relationships, promote personal strengths, encourage a sense of control, and find meaning in life (Vos et al., 2019). Baudry (2018) parted from the hypothesis that people with higher EI may be more likely to understand, regulate, and cope with daily stressors, and after their published systematic review, they concluded that higher scores of EI are associated with better mental, physical, and general health in both clinical and healthy populations. They explained it by a better use of proactive self-care health practices and greater social support resources.
Study Limitations
Some weaknesses of our study are the size of the sample and the heterogeneity among participants in terms of gender, age, cause of ABI and relationship to the patient. Therefore, further studies with a larger and more homogeneous sample should be performed. Other limitation is the absence of a control group or maybe psychometric characterization or our sample previously to the caregiver condition. Second point is difficult to achieve but the assessment of a control group could be an affordable goal for future research projects. Nevertheless, this study can be considered a starting point to other observational studies with larger sample looking forward results generalization.
CONCLUSIONS
Perceived EI is strongly correlated to resilient resources and mental health of caregivers. And all of them, EI, mental health and resilience, increase the positiveness of emotions they experienced in daily life. In addition, emotional repair, mental health, and resilience reduce negative emotions and overload. Overload increase daily negative emotions, and negative emotions associate lower resilience, emotional repair, and mental health. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical Concerns
The study was conducted according to the guidelines of the Declaration of Helsinki. This project was sent to evaluation by Ethics Committee from Hospital Regional Universitario de Málaga, Spain. Ethics committee reference: 2674-N-20. Informed consent was obtained from all subjects involved in the research.
REFERENCES
Alonso, J., Prieto, L., & Antó, J. M. (1995). La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): un instrumento para la medida de los resultados clínicos. Medicina Clínica, 104(20), 771–776.
Baudry, A. S., Grynberg, D., Dassonneville, C., Lelorain, S., & Christophe, V. (2018). Sub- dimensions of trait emotional intelligence and health: A critical and systematic review of the literature. Scandinavian Journal of Psychology, 59(2), 206–222. https://doi.org/10.1111/sjop.12424
Bryony, K., & Sharman, R. (2015). Caregivers' support needs and factors promoting resiliency after brain injury. Brain Injury, 29(9), 1082–1093. https://doi.org/10.3109/02699052.2015.1018323
Campbell-Sills, L., & Stein, M. B. (2007). Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. Journal of Traumatic Stress, 20(6), 1019–1028. https://doi.org/10.1002/jts.20271
Cornelius-White, J. (2007). Learner-centered teacher-student relationships are effective: A meta-analysis. Review of Educational Research, 77(1), 113–143. https://doi.org/10.3102/003465430298563
Díaz-García, A., González-Robles, A., Mor, S., Mira, A., Quero, S., García-Palacos, A., Baños, R., M., & Botella, C. (2020). Positive and Negative Affect Schedule (PANAS): Psychometric properties of the online Spanish version in a clinical sample with emotional disorders. BMC Psychiatry, 20, Article 56. https://doi.org/10.1186/s12888-020-2472-1
Dubey, S., Biswas, P., Ghosh, R., Chatterjee, S., Dubey, M. J., Chatterjee, S., Lahiri, D., & Lavie, C. J. (2020). Psychosocial impact of COVID-19. Diabetes & Metabolic Syndrome: Clinical Research and Reviews, 14(5), 779–788. https://doi.org/10.1016/j.dsx.2020.05.035
Faye, C., Mcgowan, J. C., Denny, C. A., & David, D. J. (2018). Neurobiological mechanisms of stress resilience and implications for the aged population. Current Neuropharmacology, 16(3), 234–270. https://doi.org/10.2 174/1570159X15666170818095105
Fernández-Berrocal, P., Extremera, N., & Ramos, N. (2004). Validity and reliability of the Spanish modified version of the Trait Meta-mood Scale. Psychological Reports, 94, 751–755. https://doi.org/10.2466/pr0.94.3.751-755
Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden- and-build theory of positive emotions. American Psychologist, 56(3), 218–226. https://doi.org/10.4135/9781412956253.n75
Gebhardt, M. C., McGehee, L. A., Grindel, C. G., & Testani-Dufour, L. (2011). Caregiver and nurse hopes for recovery of patients with acquired brain injury. Rehabilitation Nursing Journal, 36(1), 3–12. https://doi. org/10.1002/j.2048-7940.2011.tb00059.x
Hoeffding, L. K., Nielsen, M. H., Rasmussen, M. A., Norup, A., Arango-Lasprilla, J. C., Kjær, U. K., Burgdorf, K. S., Quas, K. J., & Schow, T. (2017). A manual-based vocational rehabilitation program for patients with an acquired brain injury: Study protocol of a pragmatic randomized controlled trial (RCT). Trials, 18, Article 371. https://doi.org/10.1186/s13063-017-2115-0
Karpa, J., Chernomas, W., Roger, K., & Heinonen, T. (2020). Families' experiences living with acquired brain injury: "Thinking family". A nursing pathway for family-centered care. Nursing Research and Practice, 2020, Article 8866534. https://doi.org/10.1155/2020/8866534
Knox, L., Douglas, J. M., & Bigby, C. (2015). 'The biggest thing is trying to live for two people': Spousal experiences of supporting decision-making participation for partners with TBI. Brain Injury, 29(6), 745–757. https:// doi.org/10.3109/02699052.2015.1004753
Kong, L., Liu, Y., Li, G., Fang, Y., Kang, X., & Li, P. (2016). Resilience moderates the relationship between emotional intelligence and clinical communication ability among Chinese practice nursing students: A structural equation model analysis. Nurse Education Today, 46, 64–68. https:// doi.org/10.1016/j.nedt.2016.08.028
Kreutzer, J. S., Marwitz, J. H., Sima, A. P., Mills, A., Hsu, & N., Lukow II, H. R. (2018). Efficacy of the resilience and adjustment intervention after traumatic brain injury: A randomized controlled trial. Brain Injury, 32(8), 963–971. https://doi.org/10.1080/02699052.2018.1468577
Liu, Y., Dokos, M., Fauth, E. B., Lee, Y. G., & Zarit, S. H. (2019). Financial strain, employment, and role captivity and overload over time among dementia family caregivers. The Gerontologist, 59(5), e512–e520. https://doi. org/10.1093/geront/gnz099
LoMartire, R., Äng, B. O., Gerdle, B., & Vixner, L. (2020). Psychometric properties of Short Form-36 Health Survey, EuroQol 5-dimensions, and Hospital Anxiety and Depression Scale in patients with chronic pain. Pain, 161(1), 83–95. https://doi.org/10.1097/j.pain.0000000000001700
Lond, B. J., & Williamson, L. R. (2018). "Stuck in a loop of fear": A phenomenological exploration of carers' experiences supporting a spouse with acquired brain injury. Disability and Rehabilitation, 40(24), 2907– 2915. https://doi.org/10.1080/09638288.2017.1363299
Notario-Pacheco, B., Solera-Martínez, M., Serrano-Parra, M. D., Bartolomé- Gutiérrez, R., García-Campayo, J., & Martínez-Vizcaíno, V. (2011). Reliability and validity of the Spanish version of the 10-item Connor- Davidson Resilience Scale (10-item CD-RISC) in young adults. Health and Quality of Life Outcomes, 9, Article 63. https://doi. org/10.1186/1477-7525-9-63
Rapport, L. J., Wong, C. G., & Hanks, A. (2020). Resilience and well-being after traumatic brain injury. Disability and Rehabilitation, 42(14), 2049–2055. https://doi.org/10.1080/09638288.2018.1552327
Riley, G. A. (2016). The partner's experience of traumatic brain injury and its recovery. Concussion, 1(3), CNC18. https://doi.org/10.2217/cnc- 2016-0012
Salovey, P., & Mayer, J. D. (1990). Emotional intelligence. Imagination, Cognition and Personality, 9(3), 185–211. https://doi.org/10.2190/2FDUGG-P24E-52WK-6CDG
Sánchez, M. T., Montañés, J., Latorre, J. M., & Fernández-Berrocal, P. (2006). Análisis de las relaciones entre la Inteligencia Emocional Percibida y la salud mental en la pareja. Ansiedad y Estrés, 12(2–3), 343–353.
Schweder, S., & Raufelder, D. (2019). Positive emotions, learning behavior and teacher support in self-directed learning during adolescence: Do age and gender matter? Journal of Adolescence, 73, 73–84. https:// doi.org/10.1016/j.adolescence.2019.04.004
Vos, L., Poritz, J. M. P., Ngan, E., Leon-Novelo, L. L., & Sherer, M. (2019). The relationship between resilience, emotional distress, and community participation outcomes following traumatic brain injury. Brain Injury, 33(13), 1615–1623. https://doi.org/10.1080/02699052.2019.1658132
Yu, Y., Liu, Z.-W., Zhou, W., Zhao, M., Qiu, D., Li, Y.-L., & Xiao, S.-Y. (2019). Cutoff of the Zarit Burden Interview in predicting depression and anxiety. Quality of Life Research, 28(9), 2525–2533. https://doi. org/10.1007/s11136-019-02208-7
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist, 20(6), 649–655. https://doi.org/10.1093/geront/20.6.649