Original
Stress and coping in times of pandemic: Longitudinal follow-up of a group of medical patients
Francesc Maestre-Lorén (a, Xavier López-i-Martín (b, José A. Castillo-Garayo (ab, Marco Cosentino (c
a) Clinical Psychology Department, Fundació Puigvert, Barcelona, Spain
b) FPCEE Blanquerna, Universitat Ramon Llull, Barcelona, Spain
c) Urology Andrology Department, Casa di cura Villa Maria, Padova, Italy
Ansiedad y Estrés, (2022), 22(2), 115-121
https://doi.org/10.5093/anyes2022a13
https://www.ansiedadyestres.es
Bibliography reference
INFO ARTICLE
Received 28 September 2021
Accepted 5 March 2022
Available online 21 March 2022
ABSTRACT
The Covid-19 pandemic has impacted the mental health and medical care of patients with pre-existing conditions. We longitudinally evaluated perceived stress, psychological distress, and coping strategies in 50 patients with medical diseases, finding that, 6 months after baseline evaluation, perceived stress and psychological distress were increased, and that less use was made of active coping strategies. Age (younger patients), previous psychological problems, and altered medical treatments emerge as risk factors. Proactive detection of psychopathological suffering is essential to prevent a parallel mental health pandemic from unfolding. Covid-19 has had an impact on patients with medical diseases, expressed in increased psychological vulnerability that may interfere in their disease course. While telematic monitoring is an important factor in reducing impact, early detection of psychopathological symptoms is crucial to ensuring adherence to treatments and to developing effective biopsychosocial approaches.
KEYWORDS
Covid-19
stress
Coping strategies
Psychopathological distress
Emotional health
Estrés y afrontamiento en tiempos de pandemia: Seguimiento longitudinal de un grupo de pacientes médico
Ansiedad y Estrés, (2022), 22(2), 115-121
https://doi.org/10.5093/anyes2022a13
https://www.ansiedadyestres.es
Bibliography reference
RESUMEN
La pandemia de Covid-19 ha afectado la salud mental y la atención médica de pacientes con afecciones preexistentes. Se evaluó longitudinalmente la percepción de estrés, malestar psicológico y estrategias de afrontamiento en 50 pacientes con patologías médicas, encontrándose que, 6 meses después de la evaluación inicial, el estrés percibido y el malestar psicológico se incrementaron, mientras que se redujo el uso de estrategias de afrontamiento activas. La edad (pacientes más jóvenes), los problemas psicológicos previos y la alteración del tratamiento médico emergen como factores de riesgo. La detección proactiva del sufrimiento psicopatológico es esencial para evitar que se desarrolle una pandemia paralela de salud mental. La Covid-19 ha tenido un impacto en pacientes con enfermedades médicas, expresado en una mayor vulnerabilidad psicológica que puede interferir en el curso de su enfermedad. Si bien el monitoreo telemático es un factor importante para reducir el impacto, la detección temprana de los síntomas psicopatológicos es crucial para garantizar la adherencia a los tratamientos y para desarrollar enfoques biopsicosociales efectivos.
PALABRAS CLAVE
Covid-19
Estrés
Estrategias de afrontamiento
Malestar psicopatológico
Salud emocional
Introduction
The Covid-19 pandemic is causing enormous changes affecting many facets of life. For entire populations, the pandemic entails restrictions on mobility, loss of contact with family and friends, and the need to adapt to teleworking and online teaching. The socioeconomic impact and the loss of loved ones exacerbate the emotional pain. The pandemic has generated feelings of uncertainty, vulnerability, fear, stress, and ultimately, a sensation of foreboding resulting in psychological suffering (Ornell et al., 2020; Paric et al., 2020; Taylor, 2019; Wang et al., 2020).
The knowledge acquired in the current and previous pandemics indicates that the impact on mental health will be greater than the impact on physical health (Douglas et al., 2009; Ornell et al., 2020; Taylor, 2019). The effects of Covid-19 on mental health are becoming increasingly visible, to the point of taking shape as a parallel pandemic (Vigo et al., 2020). While a fear of infection affects part of the population, the impact of measures to stop infection is more widespread, in that measures like lockdown affect the entire population, generating symptoms of stress, insomnia, anxiety, and depression (Becerra et al., 2020; Hawryluck et al., 2004; Rubin & Wessely, 2020). Wang et al. (2020), in a study conducted with a general population after 2 weeks of lockdown, reported that 54% of survey respondents reported significant psychological distress, while 29% and 17% reported anxiety and moderate or severe depression, respectively. The Covid-19 pandemic is acknowledged to be associated with stress factors that go far beyond lockdown to cause a broader and more enduring spectrum of symptoms, including confusion, moodiness, irritability, anger, insomnia, emotional exhaustion, post-traumatic stress disorder, anxiety, and depression (Brooks et al., 2020; Günther-Bel et al., 2020; Ornell et al., 2020; Paric et al., 2020; Qiu et al., 2020; Salari et al., 2020; Sandín et al., 2020).
One of the few longitudinal studies carried out on the emotional impact of the pandemic (González-Sanguino et al., 2021) was based on three evaluations carried out for a period of 2.5 months (21 March to 4 June), from the lockdown to the first de-escalation restrictive measures; while depression, anxiety, and post-traumatic stress symptoms decreased over time, the decrease was only statistically significantly for depression. Shamblaw et al. (2021) also reported a decrease in anxiety and depression symptoms between two evaluations carried out at the end of April and the end of May 2020.
Greater or lesser inference by the Covid-19 pandemic in psychological functioning depends on the presence of both risk factors and protective factors. Awareness of those factors can help identify especially vulnerable groups so that suitable public health measures can be designed aimed at mitigating the psychosocial impact of the pandemic (Bish & Michie, 2010).
Risk factors that increase emotional vulnerability and levels of anxiety, stress, and depression especially include excessive exposure to news, illness and health-related worries, unemployment, low income, age (18-40 years), single parenthood, lack of social support, loneliness, and grief for lost loved ones (Becerra et al., 2020; Bo et al., 2020; Dávila & González, 2009; Douglas et al., 2009; Paric et al., 2020; Ramírez et al., 2021; Salari et al., 2020; Smith et al., 2009; Wang et al., 2020). The emergence of psychological symptoms during the pandemic is a risk factor, since symptoms that become clinically severe, persist over time, or interfere with daily life can lead to a mental disorder, and may also affect behaviours and attitudes to anti-contagion measures (Wang et al., 2020). Substance abuse and a pre-existing psychopathological history both increase the probability of experiencing symptoms in the 4-6 months after lockdown (Douglas et al., 2009; Paric et al., 2020; Vigo et al., 2020), due to existing vulnerability and difficulties in accessing professional help (Shultz et al., 2015).
People with pre-existing physical health problems are undoubtedly more vulnerable (Cullen et al., 2020; Parpa, et al., 2015), as the focus on Covid-19-related healthcare has led to delayed diagnoses and interventions (Bakouny et al., 2021; Domínguez-Gil et al., 2020), leading to worsening physical or mental conditions, and illnesses being maintained at a subclinical level. Our specific focus, as will be seen in the empirical part of this study, was to evaluate the specific impact of the Covid-19 pandemic on patients with urology, nephrology, or andrology conditions.
As for protective factors, dyadic adjustment was found to be greater in partner relationships, while the effects of lockdown on family relationships was broadly positive (Günther-Bel et al., 2020). Social support and clear information that enabled correct interpretation of Covid-19 symptoms increased resilience and adaptive capacity (Paric et al., 2020). In the case of health professionals, an important protective factor was feeling supported by colleagues and by the employing institution (Brooks et al., 2020).
Coping strategies can be either a risk factor or a protective factor, since they mediate the emotional impact caused by stress (Lazarus & Folkman, 1984). Coping strategies (Dawson & Golijani-Moghaddam, 2020; Shamblaw et al., 2021) can be classified as: (1) avoidant coping, characterized by self-distraction, denial, substance abuse, disengagement, and self-blame; and (2) active coping, characterized by addressing difficulties, seeking support, planning, and restructuring problems in a constructive way. Quality of life is preserved by coping that is flexible and context-adjusted, and that does not lose sight of medium- and long-term objectives. In contrast, psychological distress, aggravated by a rigid pattern of coping, constitutes a risk factor for developing mental disorders (Wang et al., 2020). In their longitudinal study carried out in the context of the Covid-19 pandemic, Shamblaw et al. (2021) observed that avoidant coping was associated with greater anxiety and depression, while active coping, especially positive re-appraisal, was linked to psychological wellbeing. In that study, however, it was also observed that some active coping strategies are not effective in coping with a pandemic, and vice versa; planning, for instance, despite being an active coping strategy, is associated with greater anxiety, as thinking ahead about steps and strategies to overcome stressful situations is not useful in tackling the unpredictability of a pandemic. Care also needs to be taken with distraction strategies when they involve connecting to social media and checking news, as there is a danger of information overload about the pandemic. Excessive exposure to news when combined with a low tolerance for uncertainty has been reported to aggravate the psychological impact of the pandemic (Sandín et al., 2020).
Knowing that the pandemic causes psychological distress and stress, that coping strategies play a key role, and that people with health problems are particularly vulnerable, the aim of this longitudinal study was to evaluate how psychological distress, perceptions of stress, and coping strategies evolved in a group of patients with urological, nephrological, or andrological conditions. We also analysed whether age, psychological disorders, or affected treatment/follow-up of active medical pathologies were variables related to emotional well-being and coping strategies. Specifically, in comparing 2 evaluations separated by 6 months (T1 and T2), we hypothesize that patients will experience increased psychological distress (hypothesis 1) and greater perceived stress (hypothesis 2), and the coping strategies used will be modified (hypothesis 3).
Method
Procedure
A longitudinal study was carried out with outpatients of the Hospital Fundació Puigvert (Barcelona), using data collected for 2 periods: T1, April-May 2020 (during the lockdown mandated in the first Covid-19 wave); and T2, October-November 2020 (during the second Covid-19 wave, this time without lockdown). Once the study was approved by the hospital’s research ethics committee, participants were recruited during visits carried out telematically during lockdown. Inclusion criteria to participate in the study were: (a) to be patients in active follow-up at the hospital for any of the medical pathologies treated in the centre (urology, nephrology, andrology); (b) to be over 18 years of age; and (c) to provide written consent to participate in the research. Having language difficulties in understanding the questionnaires was the only exclusion criterion. Participants were informed of the purpose of the study, signed an informed consent, and completed the questionnaire at baseline; 6 months later, they were contacted again by telephone and asked to complete the same questionnaires. The participants did not receive any compensation for their participation in the study.
Participants
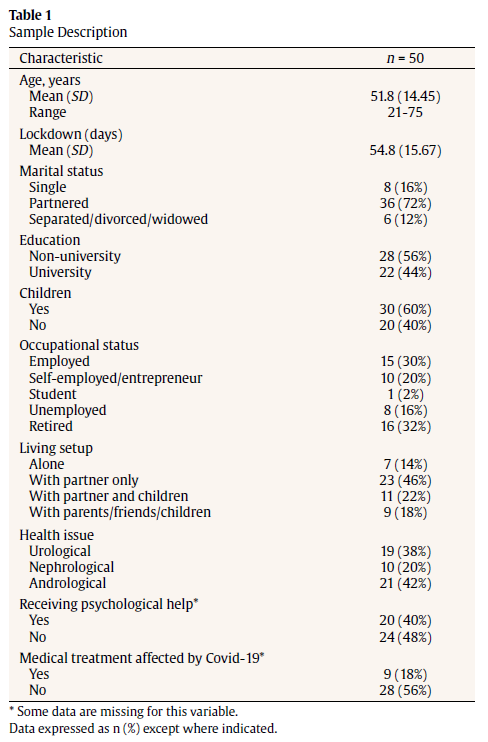
Of the 270 patients invited to participate in the study, 95 agreed. Most patients who declined to participate stated that it was due to a lack of computer skills and/or technology to access the questionnaires. Of the 95 patients, 50 who completed the questionnaires in both T1 and T2 made up the final sample, composed of 41 men and 9 women, aged between 21 and 75 years (M=51.8; SD=14.45), with urological (38%), nephrological (20%), and andrological (42%) disorders. Detailed information on the sample is reported in Table 1.
Measures
Sociodemographic data. Ad hoc questions covered age, sex, marital status, children, education, occupational status, and living setup, as well as questions specific to the study objective, such as the number of days in lockdown, affected medical treatments, and whether the respondent was receiving psychological treatment at the beginning of the pandemic.
Clinical Outcomes in Routine Evaluation-Outcome Measure (CORE-OM, Feixas et al., 2012). This self-report questionnaire, consisting of 34 items scored on a 5-point scale (ranging from ‘not at all’ to ‘most or all of the time’), assesses 4 psychological distress dimensions: subjective well-being/discomfort (4 items); problems/ symptoms (12 items, measuring anxiety, depression, trauma, and physical symptoms); life functioning (12 items, assessing intimate relationships, social relationships, and levels of daily functioning); and risk (6 items serving as clinical indicators of suicide attempts, self-harm, or acts of aggression against others). The cut-off points for mild, medium, moderate, and severe discomfort are scores of 10, 15, 20, and 25, respectively. The internal consistency of the psychometric properties of this test is satisfactory (Cronbach’s ?=0.75-0.90). Developed initially to monitor mental health treatment outcomes, it has more recently been used also to assess the impact of the pandemic on mental health (Dalise et al., 2021; Zibetti et al., 2021).
Perceived Stress Scale (PSS, Remor, 2006). This self- report instrument assesses the perceived level of stress in the previous month. It consists of 14 items scored on a 5-point scale (ranging from ‘never’ to ‘very often’), with higher scores indicating higher perceived stress. The scale does not establish cut-off points between the general population and the clinical population. In terms of psychometric properties, it has been demonstrated to have acceptable reliability (Cronbach’s ?=0.81).
Coping Strategies Questionnaire (Cuestionario de Afrontamiento del Estrés, CAE, Sandín & Chorot, 2003). This 42-item self-report measure assesses 7 basic coping strategies for stressful life situations: problem-solving, negative self-focus, positive re-appraisal, overt emotional expression, avoidance, social support, and religion. Scored on a 5-point scale (ranging from ‘never’ to ‘almost always’), higher scores for strategies indicate greater deployment of a strategy in the management of stress. Individual subscale reliabilities are acceptable (Cronbach’s ?=0.64-0.92).
Data analysis
We first compared the participants who only completed the questionnaire at baseline (T1) with the participants who completed both questionnaires (at T1 and T2) to evaluate possible differences that could affect the results. We then compared the final sample of 50 participants, at both the descriptive level (providing percentages and/or odds ratios) and the inferential level (through group comparison tests for paired samples). Finally, we used bivariate correlation to evaluate a possible association between age and the study variables, and group comparison tests for independent samples to evaluate the differential impact on patients in psychological treatment or whose medical treatments were affected by the pandemic.
Analyses were conducted using the Statistical Package for the Social Sciences (SPSS) Version 18 (IBM Corporation, Armonk, NY, USA).
Results
The final sample consisted of 50 hospital outpatients who completed questionnaires in both T1 and T2 (Table 1). No statis-tically significant differences in sociodemographic variables or in CORE-OM, PSS, or CAE responses were found for the 45 patients who responded only in T1 compared to the 50 patients who res¬ponded in both T1 and T2 (p>.05). The only statistically significant difference between the groups was the mean number of lock-down days: 55 days (8 weeks) for the former vs 63 days (9 weeks) for the latter (p=.006).
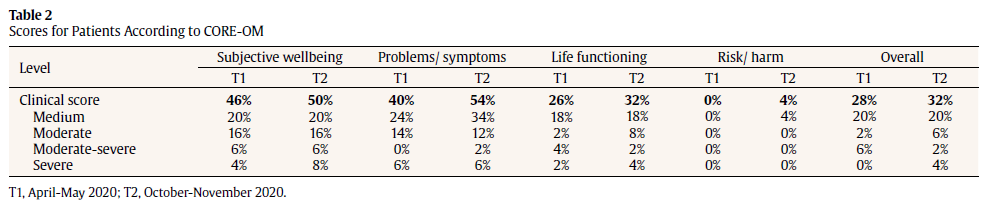
Psychological distress
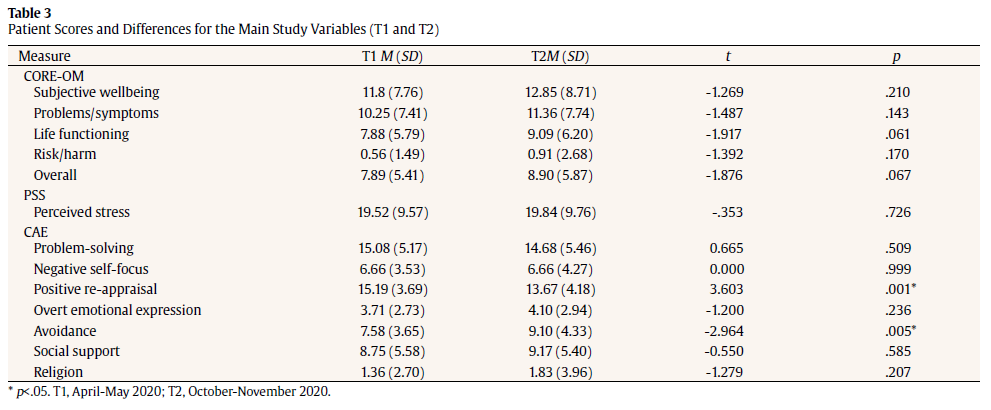
Table 2 shows the percentage of patients who obtained clinically significant CORE-OM scores in T1 and T2, broken down by degree of severity. In the initial months of the pandemic (T1), 28% of the sample presented with clinical levels of overall distress, increasing to 32% (OR=1.21; CI=0.51-2.85) 6 months later (T2). An increase was evident in all CORE-OM subscales, most markedly in the problems/ symptoms subscale (OR=1.76; CI=0.80-3.89), although differences in mean scores were not statistically significant (see Table 3).
Psychological distress in T2 was found to be negatively correlated with age, both overall (r=-.335; p=.017), for the subjective wellbeing subscale (r=-.334; p=.018), and for the life functioning subscale (r=-.313; p=.027); in T1, this negative correlation was only evident for the subjective wellbeing subscale (r=-.337; p=.019).
Perceived stress
There were no significant differences in mean scores for stress as measured by the PSS between T1 and T2: 19.52 vs 19.84 (p=.726). If we take, as a benchmark, the questionnaire validated for Spanish (Remor, 2006), where a mean score of 25 was obtained for a non-clinical population, the scores for our sample did not seem to reflect a major level of stress. However, considering the stress level of individual patients, 14% and 20% obtained scores higher than 25 in T1 and in T2, respectively (OR=1.54; CI=0.53-4.42). Once again a correlation with age was evident, but only for T2 (r=-.383; p=.007).
Coping strategies
The most widely used coping strategies were observed to be problem-solving, followed by positive re-appraisal in both T1 and T2 (Table 3). By T2, statistically significant changes were evident in the deployment of 2 coping strategies in particular: use of positive re-appraisal (p=.001) was reduced, and use of avoidance (p=.005) was increased.
With respect to age, compared to older people, younger people made greater use of social support search strategies in T1 (r=¬.352; p=.013) and of avoidance strategies in T2 (r=-.351; p=.012).
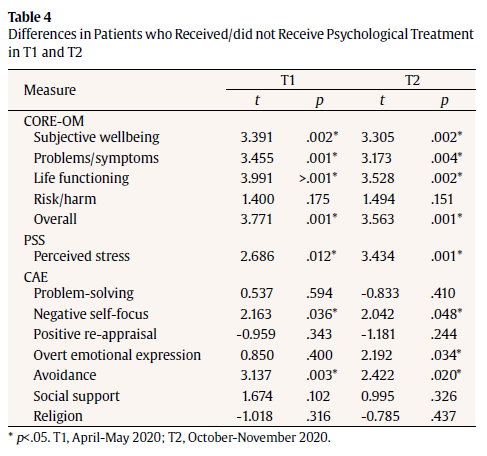
Psychological treatment
A more detailed analysis of the characteristics of the sample pinpointed differences in psychological distress and perceived stress as experienced during the Covid-19 pandemic by patients with urological, nephrological, or andrological conditions. In T1 and T2, patients who received, compared to those who did not receive, psychological treatment showed significantly higher levels of distress (CORE-OM) and stress (PSS), and relied more on coping strategies based on negative self-focus, avoidance, and overt emotional expression (Table 4).
Medical attention
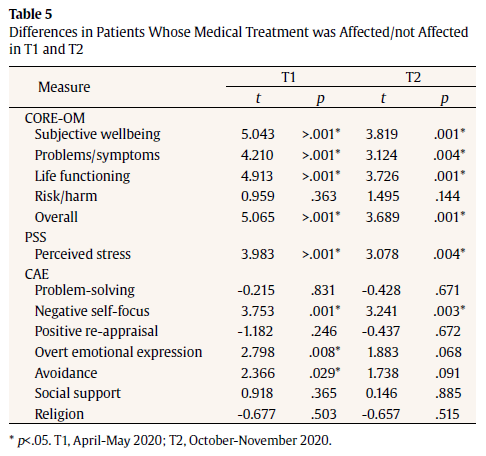
The subgroup of people who reported that their medical treatments were affected in both T1 and T2 showed significantly higher levels of psychological distress and perceived stress; they were also observed to more frequently use coping strategies based on negative self-focus, and also initially, overt emotional expression and avoidance (Table 5).
Discussion
The objective of this study was to longitudinally evaluate psychological distress, perceived stress, and coping strategies of patients with urological, nephrological, or andrological diseases during the Covid-19 pandemic. Despite the specificity of the pathologies included in the study, our findings regarding the psychological impact of the pandemic can be considered representative of what may be experienced by patients with other acute or chronic medical pathologies, whose hospital treatment and relationship with their doctor has been affected.
The first evaluation was carried out in April-May 2020 (T1), i.e., during the initial lockdown aimed at bringing the pandemic under control, and the second evaluation was carried out 6 months later, in October-November 2020 (T2). In T1 and T2, 95 and 50 patients responded, respectively, with the duration of lockdown as the only statistically significant difference between the 2 groups (slightly shorter for the former).
Perceived stress, as a whole, remained at normal levels in the final sample of 50 patients, although by T2, a fifth reported higher than average stress scores. Psychological distress (measured by CORE-OM) increased in the 6 months between the T1 and T2 evaluations, especially reflected in the psychological symptoms subscale. By T2, almost a third of patients reported clinically significant psychological distress. Hypothesis 1 (increased psychological distress) is therefore confirmed, but not hypothesis 2 (greater perceived stress).
This finding of increased psychological distress contradicts other studies that reported a decrease (González-Sanguino et al., 2021; Shamblaw et al., 2021). We suggest that the discrepancy is attributable to various factors. First, our study was carried out with a vulnerable group of people receiving medical treatment for a pre-existing condition (Cullen et al., 2020). A second difference is that the other longitudinal studies took place over shorter periods than our 6 months, e.g., 4 weeks for Shamblaw et al. (2021). Finally, data in our study and the other studies were collected at different times; we collected our T2 data during a new wave of infections, when pandemic fatigue was growing and there was no indication that vaccines would be available, while González-Sanguino et al. (2021) collected data twice during lockdown and again during de-escalation towards the so-called ‘new normal’.
Although the incidence of distress increased, the pandemic had a mild impact on most patients in our sample. Leaving aside the possible incidence of key factors that cushioned the impact, such as family support (Günther-Bel et al., 2020), most of our patients did not feel that their medical care had been adversely affected, even though face-to-face visits were very restricted and largely replaced by telematic contact. The fact that contact is maintained has been reported to mitigate feelings of abandonment and to preserve accessibility, therapeutic bond, and institutional containment (Sosnowski et al., 2020).
Coping strategies may play a role in stress mitigation. Problem-solving and positive re-appraisal were the most widely used strategies by our respondents, together with those that researchers associate with adaptability (Dawson & Golijani-Moghaddam, 2020; Shamblaw et al., 2021). Positive re-appraisal involves considering favourable aspects of a situation, being optimistic, and appropriately re-assessing the experience. The longitudinal nature of our study allowed us to observe that, with the passage of time, coping strategies are modified (confirming hypothesis 3). While a problem-solving strategy was maintained (complying with rules, social distancing, mask use, hand hygiene), the use of positive re-appraisal was reduced, as evidenced by less faith in the fact that ‘everything will turn out fine’. Strict mobility and social distancing regulations meant that the key coping strategy of seeking social support was highly restricted. Avoidance as a coping strategy increased in T2, especially among younger people. In the context of a pandemic of uncertain duration, the ability to deploy a wide range of coping strategies is adaptive – even when it includes strategies considered less effective by the literature (Dawson & Golijani-Moghaddam, 2020).
If the health and socioeconomic crisis, as it would seem, is prolonged in time, then the risk increases of coping strategies becoming undermined and ineffective, with the consequent increase in suffering. Our findings corroborate existing research (Becerra et al., 2020; Bo et al., 2020; Dávila & González, 2009; Douglas et al., 2009; Paric et al., 2020; Ramírez et al., 2021; Salari et al., 2020; Smith et al., 2009; Wang et al., 2020) in suggesting that younger people tend to experience greater psychological distress and perceived stress. This may be because our younger patients, with less experience in managing their urological, nephrological, or andrological disease, view the pandemic scenario as more uncertain and worrying.
Patients with previous psychological difficulties and those whose medical treatment is affected by the pandemic are also more vulnerable (Paric et al., 2020). Our patients reported greater stress and more psychological distress, while coping strategies characterized by negative self-focus, avoidance, and overt emotional expression were increasingly deployed over time.
Proactive detection of psychopathological suffering is essential to prevent a parallel mental health pandemic from adding to the Covid-19 pandemic (Vigo et al., 2020). Younger patients with a psychopathological history whose medical treatment is affected should be considered a population at risk and be prioritized for preventive psychological care. It is important to develop specific types of intervention (supportive, expressive, or mixed), adapted to individual and community needs, to help people recover psychological functioning and avoid the chronification of pre-existing disorders (Bitanihirwe, 2016). It is also important, for both people with health conditions and the population as a whole, to strengthen self-care resources and family and social support systems (Tizón, 2020; Vigo et al., 2020).
As for the limitations of our study, the sample cannot be considered representative of the patients treated in our hospital; furthermore, patients lacking computer resources or skills were underrepresented (mainly elderly people). Since our study only covered the first 7-8 months of the pandemic, it does not reflect socioeconomic and mental health effects that have yet to emerge in their full intensity. While patients were asked if they were receiving psychological treatment, there was no question to establish since when, which would have been relevant information. Finally, our findings only refer to patients with urological, nephrological, or andrological diseases, but it would undoubtedly be useful for our findings to be compared with those for people with other diseases.
Despite those limitations, our study of patients with urological, nephrological, or andrological diseases allows us to conclude that the impact of the pandemic has not necessarily implied a generalized increase in psychopathological symptoms, even though a third of our respondents did present with clinically significant distress. The risk factors that emerged in our study were age (younger patients), a history of psychological problems, and affected medical treatments. Bearing in mind that psychological factors not only affect general physical health, but also the evolution of the pandemic, further research is essential to prepare for the future. As pointed out by the philosopher Josep M. Esquirol (2020), the Covid-19 pandemic should be a spur to reinforcing a genuine human capacity for care, both at the individual, family, social, and, of course, healthcare level.
References
Bakouny, Z., Paciotti, M., Schmidt, A. L., Lipsitz, S. R., Choueiri, T. K., & Trinh, Q.-D. (2021). Cancer Screening Tests and Cancer Diagnoses During the COVID-19 Pandemic. JAMA Oncology, 7(3), 458–460. https://doi.org/10.1001/jamaoncol.2020.7600
Becerra-García, J.A., Giménez Ballesta, G., Sánchez-Gutiérrez, T., Barbeito Resa, S., Calvo Calvo, A. (2020). Síntomas psicopatológicos durante la cuarentena por Covid-19 en población general española: un análisis preliminar en función de variables sociodemográficas y ambientales-ocupacionales. Rev Esp Salud Pública. 94,e1-11.
Bish, A., & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15(4), 797–824. https://doi.org/10.1348/135910710X485826
Bitanihirwe, B. K. Y. (2016). Monitoring and managing mental health in the wake of Ebola. Commentary. Annali Dell’Istituto Superiore Di Sanita, 52(3), 320–322. https://doi.org/10.4415/ANN_16_03_02
Bo, H.-X., Li, W., Yang, Y., Wang, Y., Zhang, Q., Cheung, T., Wu, X., & Xiang, Y.-T. (2020). Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychological Medicine, 1–2. https://doi.org/10.1017/S0033291720000999
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. https://doi.org/10.1016/S0140-6736(20)30460-8
Cullen, W., Gulati, G., & Kelly, B. D. (2020). Mental health in the COVID-19 pandemic. QJM: monthly journal of the Association of Physicians, 113(5), 311–312. https://doi.org/10.1093/qjmed/hcaa110
Dalise, S., Tramonti, F., Armienti, E., Niccolini, V., Caniglia-Tenaglia, M., Morganti, R., & Chisari, C. (2021). Psycho-social impact of social distancing and isolation due to the COVID-19 containment measures on patients with physical disabilities. European Journal of Physical and Rehabilitation Medicine, 57(1), 158-165. https://doi.org/10.23736/S1973-9087.20.06535-1
Dávila Quintana, C. D., & González López-Valcárcel, B. (2009). [The economic crisis and health]. Gaceta Sanitaria, 23(4), 261–265. https://doi.org/10.1016/j.gaceta.2009.04.003
Dawson, D. L., & Golijani-Moghaddam, N. (2020). COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. Journal of Contextual Behavioral Science, 17, 126–134. https://doi.org/10.1016/j.jcbs.2020.07.010
Domínguez-Gil, B., Coll, E., Fernández-Ruiz, M., Corral, E., Del Río, F., Zaragoza, R., Rubio, J. J., & Hernández, D. (2020). COVID-19 in Spain: Transplantation in the midst of the pandemic. American Journal of Transplantation : Official Journal of the American Society of Transplantation and the American Society of Transplant Surgeons, 20(9), 2593–2598. https://doi.org/10.1111/ajt.15983
Douglas, P. K., Douglas, D. B., Harrigan, D. C., & Douglas, K. M. (2009). Preparing for pandemic influenza and its aftermath: Mental health issues considered. International Journal of Emergency Mental Health, 11(3), 137–144.
Esquirol, J.M. (2020, July 19). El movimiento más radical y más humano sería el de cuidarnos. El País. https://elpais.com/ideas/2020-07-18/josep-maria-esquirol-el-movimiento-mas-radical-y-mas-humano-es-el-de-cuidarnos.html
Feixas, G., Evans, C., Trujillo, A., Saúl, L.A., Botella, L., Corbella, S., González, E., Bados, A., García E., & López, M.A. (2012). [Spanish version of the CORE-OM: Clinical Outcomes in Routine Evaluation – Outcome Measure]. Revista de Psicoterapia, 89, 109–135.
González-Sanguino, C., Ausín, B., Castellanos, M. A., Saiz, J., & Muñoz, M. (2021). Mental health consequences of the Covid-19 outbreak in Spain A longitudinal study of the alarm situation and return to the new normality. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 107. https://doi.org/10.1016/j.pnpbp.2020.110219
Günther, B. C., Vilaregut, A., Carratala, E., Torras, G. S., & Pérez, T. C. (2020). A Mixed-method Study of Individual, Couple, and Parental Functioning During the State-regulated COVID-19 Lockdown in Spain. Family Process, 59(3), 1060–1079. https://doi.org/10.1111/famp.12585
Hawryluck, L., Gold, W. L., Robinson, S., Pogorski, S., Galea, S., & Styra, R. (2004). SARS control and psychological effects of quarantine, Toronto, Canada. Emerging Infectious Diseases, 10(7), 1206–1212. https://doi.org/10.3201/eid1007.030703
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
Ornell, F., Schuch, J. B., Sordi, A. O., & Kessler, F. H. P. (2020). ‘Pandemic fear’ and COVID-19: mental health burden and strategies. Brazilian Journal of Psychiatry, 42(3), 232–235. https://doi.org/10.1590/1516-4446-2020-0008
Paric, A., Ravindran, L., & Ravindran, A. (2020). Psychological dimensions of COVID-19: Perspectives for the practicing clinician. International Journal of Noncommunicable Diseases, 5(2), 83-89. https://doi.org/10.4103/jncd.jncd_27_20
Parpa, E., Tsilika, E., Gennimata, V., & Mystakidou, K. (2015). Elderly cancer patients’ psychopathology: A systematic review Aging and mental health. Archives of Gerontology and Geriatrics, 60(1), 9–15. https://doi.org/10.1016/j.archger.2014.09.008
Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General Psychiatry, 33(2), e100213. https://doi.org/10.1136/gpsych-2020-100213
Ramírez, M. T. G., Hernández, R. L., & Berumen, L. Q. (2021). Tolerancia al estrés y satisfacción con la vida como predictores del impacto por el confinamiento debido al COVID-19. Ansiedad y Estrés, 27, 1-6. https://doi.org/10.5093/anyes2021a1
Remor, E. (2006). Psychometric Properties of a European Spanish Version of the Perceived Stress Scale (PSS). The Spanish Journal of Psychology, 9(1), 86–93. https://doi.org/10.1017/S1138741600006004
Rubin, G. J., & Wessely, S. (2020). The psychological effects of quarantining a city. BMJ (Clinical Research Ed.), 368, m313. https://doi.org/10.1136/bmj.m313
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S., & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Globalization & Health, 16(1), 1–11. https://doi.org/10.1186/s12992-020-00589-w
Sandín, B., & Chorot, P. (2003). [The Coping Strategies Questionnaire: Development and preliminary validation]. Revista de Psicopatología y Psicología Clínica, 8(1), 39–54. https://doi.org/10.5944/rppc.vol.8.num.1.2003.3941
Sandín, B., Valiente, R. M., García-Escalera, J., & Chorot, P. (2020). [Psychological impact of the COVID-19 pandemic: Negative and positive effects in Spanish people during the mandatory national quarantine]. Revista de Psicopatología y Psicología Clínica, 25(1), 1–22. https://doi.org/10.5944/rppc.27569
Shamblaw, A. L., Rumas, R. L., & Best, M. W. (2021). Coping during the COVID-19 pandemic: Relations with mental health and quality of life. Canadian Psychology/Psychologie Canadienne. https://doi.org/10.1037/cap0000263
Shultz, J.M., Baingana, F., Neria, Y. (2015). The 2014 Ebola Outbreak and Mental Health: Current Status and Recommended Response. JAMA, 313(6), 567–568. https://doi.org/10.1001/jama.2014.17934
Smith, B. W., Kay, V. S., Hoyt, T. V., & Bernard, M. L. (2009). Predicting the anticipated emotional and behavioral responses to an avian flu outbreak. American Journal of Infection Control, 37(5), 371–380. https://doi.org/10.1016/j.ajic.2008.08.007
Sosnowski, R., Kamecki, H., Joniau, S., Walz, J., Klaassen, Z., & Palou, J. (2020). Introduction of Telemedicine During the COVID-19 Pandemic: A Challenge for Now, an Opportunity for the Future. European Urology, 78(6), 820–821. https://doi.org/10.1016/j.eururo.2020.07.007
Taylor, S. (2019). The psychology of pandemics: Preparing for the next global outbreak of infectious disease. Cambridge Scholars Publishing.
Tizón J. L. (2020). Salud emocional en tiempos de pandemia. Herder.
Vigo, D., Patten, S., Pajer, K., Krausz, M., Taylor, S., Rush, B., Raviola, G., Saxena, S., Thornicroft, G., & Yatham, L. N. (2020). Mental Health of Communities during the COVID-19 Pandemic. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie, 65(10), 681–687. https://doi.org/10.1177/0706743720926676
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., McIntyre, R. S., Choo, F. N., Tran, B., Ho, R., Sharma, V. K., & Ho, C. (2020). A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain, Behavior, and Immunity, 87, 40–48. https://doi.org/10.1016/j.bbi.2020.04.028
Zibetti, M. R., Serralta, F. B., & Evans, C. (2021). Longitudinal Distress among Brazilian University Workers during Pandemics. International Journal of Environmental Research and Public Health, 18(17), 9072. https://doi.org/10.3390/ijerph18179072