Original article
Escala de miedo a la COVID-19: Adaptación y propiedades psicométricas en población peruana
Wilson Hernández(a), Andrea Burneo(a), Mónica Cassaretto(b)
- GRADE – Grupo de Análisis para el Desarrollo
- Pontificia Universidad Católica del Perú
Ansiedad y Estrés, 27 (2021) 103-111
https://doi.org/10.5093/anyes2021a14
https://www.ansiedadyestres.es
Bibliography reference
INFORMACIÓN DEL ARTÍCULO
Recibido el 8 July 2020
Aceptado el 9 March 2021
Online el 27 September 2021
RESUMEN
Contexto y objetivo: El contexto actual causado por la COVID-19 ha cambiado la vida social y cotidiana en todo el mundo. La salud mental no es la excepción. El objetivo de este estudio fue adaptar y analizar las propiedades psicométricas de la versión peruana de la Escala de Miedo al COVID-19 (FCV-19S) en una muestra de profesionales peruanos.
Material y métodos: La muestra estuvo compuesta por 169 participantes de un estudio longitudinal sobre el síndrome de agotamiento durante la pandemia en Perú. Se realizó el método de traducción inversa (del inglés al español). Se realizó un análisis factorial confirmatorio (AFC). Además, se llevaron a cabo análisis de confiabilidad (Alfa de Cronbach, Omega de McDonald y test-retest) y correlaciones con otras variables.
Resultados: Los resultados confirman la naturaleza unidimensional del instrumento (AFC) con excelentes indicadores de bondad de ajuste (CFI = .996; TLI = .99; RMSEA = .06; SRMR = .04) y presentan buenos niveles de confiabilidad (a = .79; ? = .81; ICC = .75). Además, se encontró evidencia de validez externa con la Escala de Estrés Traumático Secundario y la Escala de Estrés Percibido. El puntaje del FCV-19S presenta correlaciones previamente desconocidas con el miedo al contagio de familiares, el miedo de contagio en lugares públicos y la percepción de salud autoreportada. Se hallaron diferencias por género, aunque deben ser corroboradas en muestras más amplias.
Principales conclusiones. La versión peruana del FCV-19S muestra sólidas propiedades psicométricas. Su uso es atractivo para el estudio de la salud mental durante la pandemia y, el diseño y focalización de iniciativas en grupos y espacios vulnerables.
PALABRAS CLAVE
Coronavirus
COVID-19
FCV-19S
Miedo
Psicometría
Estrés
Fear of COVID-19 Scale: Adaptation and psychometric properties in Peruvian population
Ansiedad y Estrés, 27 (2021) 103-111
https://doi.org/10.5093/anyes2021a14
https://www.ansiedadyestres.es
Bibliography reference
ABSTRACT
Context and objective: Current context caused by COVID-19 has changed social and day-to-day life worldwide. Mental health is no exception. The objective of this study was to adapt and analyze the psychometric properties of the Fear of COVID-19 Scale (FCV-19S) in a sample of Peruvian professionals.
Material and methods. The sample was composed of 169 participants of a longitudinal study about burnout during the pandemic in Peru. Translation-back translation method was performed (from English to Spanish). Confirmatory factor analysis (CFA) was conducted. Additionally, reliability analyses (Cronbach's Alpha, McDonald's Omega and Test-retest) and correlations with other variables were carried out.
Results: Results confirm the one-dimensional nature of the instrument (CFA) with excellent indicators of goodness of fit (CFI = .996; TLI = .99; RMSEA = .06; SRMR = .04) and present good levels of reliability (a = .79; ? = .81; ICC = .75). Furthermore, evidence for external validity was found with the Secondary Traumatic Stress Scale and Perceived Stress Scale. The FCV-19S score presents previously unknown correlations with fear of infection of relatives, fear of infection in public places and self-reported perceived health. The score differs by gender, but further examination with larger samples are needed.
Main conclusions: The Peruvian version of the FCV-19S shows solid psychometric properties. Its use is attractive for the study of mental health during the pandemic, and the design and focalization of initiatives in vulnerable groups and spaces.
KEYWORDS
Coronavirus
COVID-19
FCV-19S
Fear
Psychometric
Stress
1. Introduction
From its origins in Wuhan, China, in November 2019 the coronavirus-19 disease (COVID-19) expanded at such high speed that only four months later, on March 11th, 2020, the World Health Organization declared it a global pandemic (WHO, 2020a). As of February 02, 2021, more than one hundred million infected persons have been reported over the world, as well as two million deaths (WHO, 2020b).
In Peru, the first case was detected on March 6th. Despite being the first South American country to adopt compulsory social distancing including an almost complete shutdown of multiple services, to date Peru finds itself within the five countries in South America with the highest rate of infected persons and deaths per capita (WHO, 2020b). In practice, social isolation and lockdown was broken progressively by citizens looking for income after job loss and economic downturn.
According to Lazarus & Folkman (1984), individuals facing stimulus will engage in an automatic evaluating the situation, known as the primary appraisal, and then to the secondary appraisal of the stressor, that leads them to an evaluation of their capacity to cope with this situation which will occasioned certain emotions, such as fear. Fear is usually adaptive and involves basic biological processes that prepare us for survival, allowing us to respond to threats with safety measures, such as escaping, distancing or flight (Reeves, 2010). This emotion arises out of the interpretation that a person gives to a situation that they consider dangerous and that constitutes a threat to their physical or psychological well-being (Folkman et al., 1986; Reeves, 2010). In the face of highly infectious diseases, a number of emotional responses can appear, such as fear, anxiety, boredom, anger, loneliness, among others (Rubin & Wessely, 2020). Fear of the disease has shown to be the most frequent response in pandemic scenarios (Pakpour & Griffiths, 2020).
In the face of COVID-19 context, risk of contagion and social isolation measures expose the population to significant risks of mental health issues. This is materialized due to the high perception of vulnerability the disease generates due to its high contagiousness and rapid spread.
Despite the proliferation of fear, mental health during COVID-19 times has received little attention (Satici et al., 2020). Recent studies have identified that the fear of COVID-19 is related to preexisting conditions such as anxiety, depression, post-traumatic stress, and suicide ideation (Bitan et al., 2020). These risks increase with exposure to social media (Gao et al., 2020) and do not tend to diminish over time, according to a longitudinal study carried out in China (Wang et al., 2020).
Studying the fear of COVID-19 would contribute towards an understanding of its relation to mental health, the need of developing prevention and support programs in general population and focalized groups, and the promotion of communicational health (Pakpour & Griffiths, 2020). It could also contribute to promote the use of interventions that support protective factors, such as social capital or coping mechanisms, that could act as buffers of depression and stress during the pandemic in China.
Due to a lack of appropriate psychometric instruments to study this phenomenon, Ahorsu et al. (2020) developed the Fear of COVID-19 Scale (FCV-19S) in Iran. With only seven items and good psychometric properties, it shows to be an instrument that is both straightforward and quick to use. Their sample was composed of 717 Iranian participants (M = 31.25; SD = 12.68). Its development was done in four phases: (a) an exhaustive review of general fear-related scales, with an outcome of 28 selected items; the evaluation of two panels of experts from different fields, where (b) the first panel maintained 17 items and (c) the second panel examined this selection, and removed seven additional items; finally, (d) this ten-item scale was used in a pilot test performed with 46 participants through individual phone-calls. Based on the results of this pilot test, three more items were removed, such that the final version of FCV-19s was obtained.
To date, it has been successfully validated in the following countries: Italy (Soraci et al., 2020), Turkey (Haktanir et al., 2020; Satici et al., 2020), Bangladesh (Sakib et al., 2020), Russia and Belarus (Reznik et al., 2020), Israel (Bitan et al., 2020), Saudi Arabia (Alyami et al., 2020), Greece (Tsipropoulou et al., 2020), New Zealand (Winter et al., 2020), United States (Perz et al., 2020), Japan (Masuyama et al., 2020) and Peru (Huarcaya-Victoria et al., 2020). Although the majority of validations have confirmed the one-dimensional structure of the FCV-19S, some of these studies, when performing an exploratory factor analysis, found two factors (Bitan et al., 2020; Reznik et al., 2020). In that regard, Pakpour et al. (2020) have criticized the data analysis of Bitan et al. (2020), arguing that it could have led to erroneous decisions related to their results and their interpretation. To our knowledge, the only studies that found a bifactorial model (CFA) to be the best fit were conducted in Japan (Masuyama et al., 2020) and Peru (Huarcaya-Victoria et al., 2020), when using Diagonally Weighted Least Squares (DWLS) and Robust ML (MLR), respectively. However, Weighted Least Square Mean and Variance Adjusted Estimators (WLSMV) is considered as the best estimation for ordinal variables (Brown, 2015). In addition, this method allows for a less restrictive model with small samples as is our case. All the above has generated a discussion about the adequacy of the factorial structure of the FCV-19S.
The present study has the objective of adapting the FCV-19S into Spanish and analyzing its psychometric properties based on the data obtained during a larger ongoing longitudinal study about burnout in professional workers of a helpline for domestic violence in Peru.
2. Material and methods
2.1. Participants
This study is framed within an ongoing larger longitudinal study about burnout during the pandemic among professional workers of a helpline for domestic violence in Peru, that belongs to the Ministry of Women and Vulnerable Population. The helpline is a free service that employs 202 operators (80% female). Measurements were conducted on the same sample (June 12th-25th 2020). The sample was composed of the 169 persons that participated (80% of the operators). Dropouts attained 18% of the sample. The age of the participants ranged from 28 to 61 years old (M = 40; SD = 8.08). Additional characteristics of the sample are given in Table 1.
The study was conducted with the approval of the Ministry, and all participants provided informed consent. The participants completed the online protocol that took in account sociodemographic variables and instruments relevant to the longitudinal study, as well as the FCV-19S itself.
Table 1

2.2. Instruments
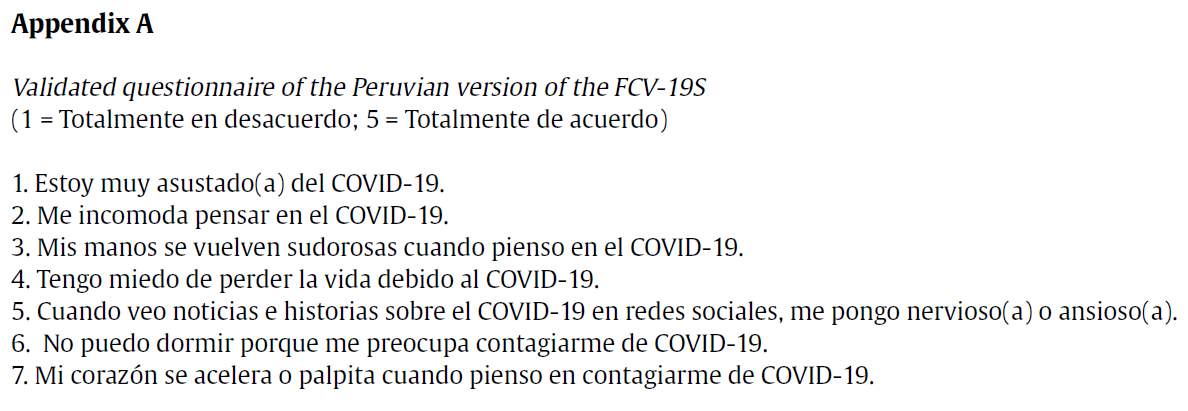
Fear of COVID-19 Scale (Ahorsu et al., 2020). This scale measures the fear related to COVID-19. This instrument contains seven items with a 5-point Likert scale format (where 1= Strongly Disagree and 5 = Strongly Agree) and the total score is obtained by simple addition, thus ranging from 7 to 35 points. A higher score will be an indicator of a higher COVID-19 related fear.
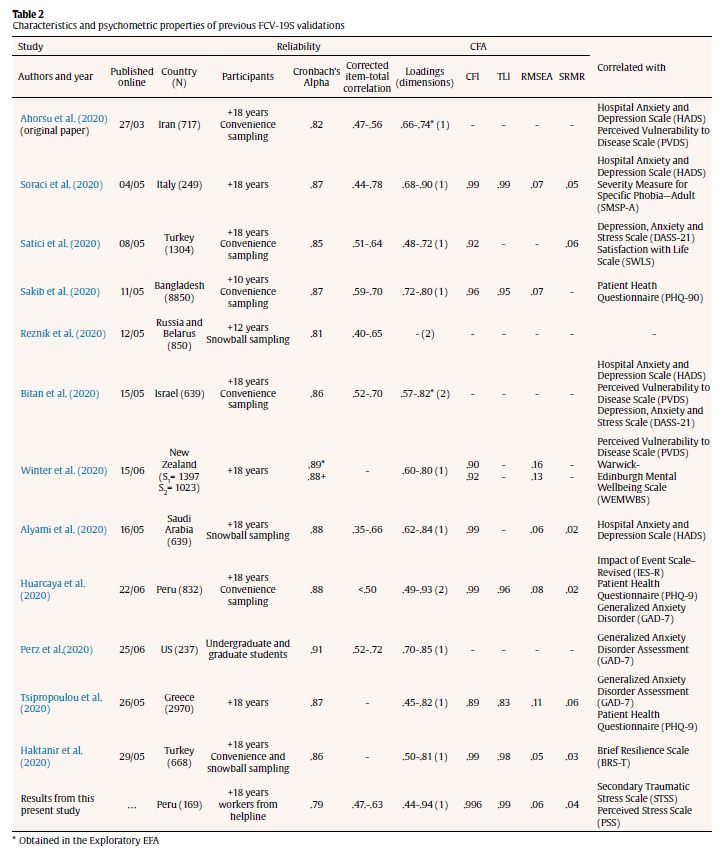
With regards to its internal structure, Ahorsu et al. (2020) reports that the FCV-19S was constituted as a one-dimensional instrument with 7 items, which had factor loadings that ranged between .66 and .74. Furthermore, reliability of evidence was obtained through Test-retest (ICC = .72), Cronbach's Alpha (.82), and corrected item-test correlations (.47-.56). Finally, significant (p < .001) and positive correlations were obtained with the sub-scales of the Persian version of the Hospital Anxiety and Depression Scale (HADS) (r anxiety = .51, r depression = .43) and the subscales of the Perceived Vulnerability to Disease Scale (r perceived infectability = .48, r germ aversion = .46). The characteristics of eleven validations of the original instrument are shown in Table 2. Overall, the psychometric properties are satisfactory and most of them (eight) confirm the one-dimensional, seven item structure of the FCV-19S.
Secondary Traumatic Stress Scale – STSS (Moreno-Jiménez et al., 2004). The Mexican validation of the STSS was employed (Meda-Lara et al., 2011). It is composed of 14 items separated in three factors: emotional fatigue, shaking up of beliefs and symptoms of secondary trauma; with a 4-point Likert scale (where 1 = Strongly Disagree and 4 = Strongly Agree). Alphas of .86, .70 and .82 were found for its three factors, respectively.
Perceived Stress Scale -PSS (Cohen et al., 1983). The Peruvian validation (Guzmán-Yacaman & Reyes-Bossio, 2018) was used, which is composed of 14 items (seven are inverse) with a five-point Likert scale format (where 0 = Never and 5 = Almost always). A .87 alpha was found.
Fear of infection of relatives. This was approached in a straightforward fashion, by means of a question ("Currently, how afraid are you that someone in your household might get infected with COVID-19?") with a 5-point Likert scale format (1= Not at all; 5 = Very much).
Fear of infection in public places. Five spaces of high influx and infection risk were identified: markets or supermarkets, small stores (pharmacies, grocery stores, etc.), public transportation, streets and workplace. For each of these, a question was asked ("What is your level of fear of getting infected with COVID-19 in the following space: ___?") with a 5-point Likert scale format (where 1 = Very Low and 5 = Very High).
Self-reported health status. This question refers to the subject's perceived health ("On a scale of 1 to 5, how would you rate your health?") with a 5-point answer scale (where 1 = Poor and 5 = Excellent).
2.3. Procedure
The first step was the translation-back translation method. It was performed independently by three psychologists with high proficiency in English. First, one of the psychologists translated the version from English to Spanish, while a second one performed a verification in cooperation with two of the co-authors of this study. The back translation of this verified version was performed by a third psychologist and was after revised by the same two co-authors.
Afterwards, a linguistic pilot with three professional workers of the helpline was carried out; no changes to the translation were suggested. In Item 5, the term "social media" was modified in favor of "redes sociales", as this term was considered to be more appropriate for our particular context. The final version of the FCV-19S is presented in the Appendix A.
Tabla - 2
2.4. Data analysis
To establish the internal structure of the FCV-19s, the CFA was conducted through the Weighted Least Square Mean and Variance Adjusted Estimators (WLSMV) estimation method. Goodness of fit indices were calculated and evaluated with the cut-offs suggested by Hu & Bentler (1999): Chi-square, Comparative Fit Index and the Tucker-Lewis Index (CFI, TLI >. 90), Root Mean Square Error Approximation and Standardized Root Mean-Square Residual (RMSEA, SRMR < .08). Afterwards, the internal consistency was tested using Cronbach's Alpha (> .7) and corrected item-test correlations were also examined (<.3). Furthermore, Omega coefficient (<.7) with correlated error was analyzed due to Cronbach's Alpha limitations (McNeish, 2018). The longitudinal study allowed us to perform a Test-retest reliability (>.5).
Finally, for external validity checks, latent correlations were estimated between the FCV-19S and both Secondary Traumatic Stress Scale and Perceived Stress Scale with the same estimation method as stated before. Furthermore, latent correlations models were estimated with three additional variables: fear of infection of relatives, fear of infection in public places and self-reported perceived health. They were considered as latent variable single indicators (Brown, 2015). For that matter, error variance was estimated taking into account the sample variance of each indicator and setting the internal consistency at .80. Cohen (1988) criteria was used: small (.10= |r| = .3), medium (.3 = |r| = .5) and large (|r| > .5).
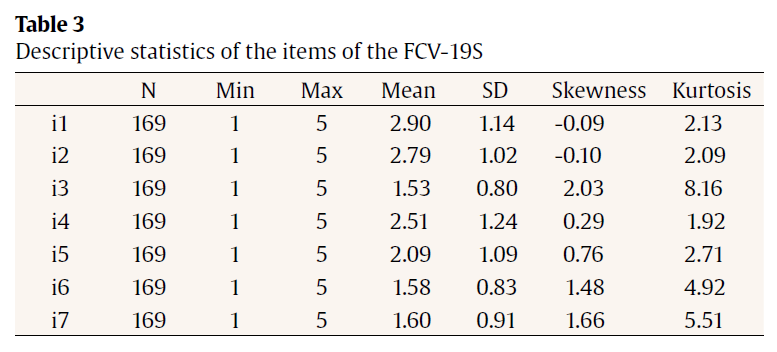
In light of the previous findings, the group comparisons (women vs men) were performed through a mean-comparison test. Descriptive statistics (Table 3) were employed to analyze the basic characteristics of the items (mean, standard deviation, minimum, maximum, skewness and kurtosis). The data were analyzed using Stata 14 and R Studio version 4.0.3.
Table 3
3. Results
3.1. Confirmatory Factor Analysis
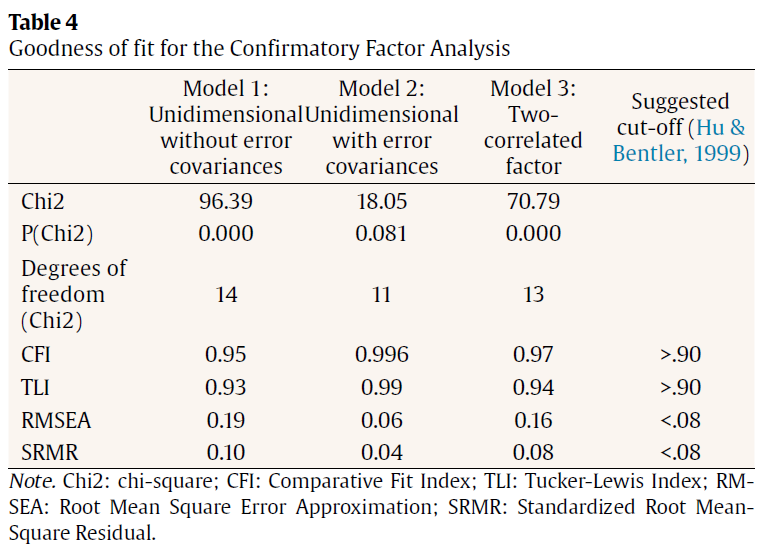
CFA was performed. Due to the ordinal nature of the 5-point Likert scale of the FCV-19S' items, Diagonally Weighted Least Squares with Mean and Variance corrected estimation method was used. Three models were tested. Model 1 is one-dimensional, and Model 2 included three error variances suggested by the modification indices (Figure 1). Model 2 presents a marked improvement of the goodness of fit indicators, which are set in adequately optimal ranges (CFI= .996, TLI= .99, RMSEA = 0.06, SRMR = .04; Table 4), with standardized factor loadings above .4. We also tested a two-correlated factor (Model 3), but the high correlation between the two factors (.82) suggested a unidimensional model. Lastly, the bifactor model did not converge. Only two previous study reports this type of model.
Figure 1
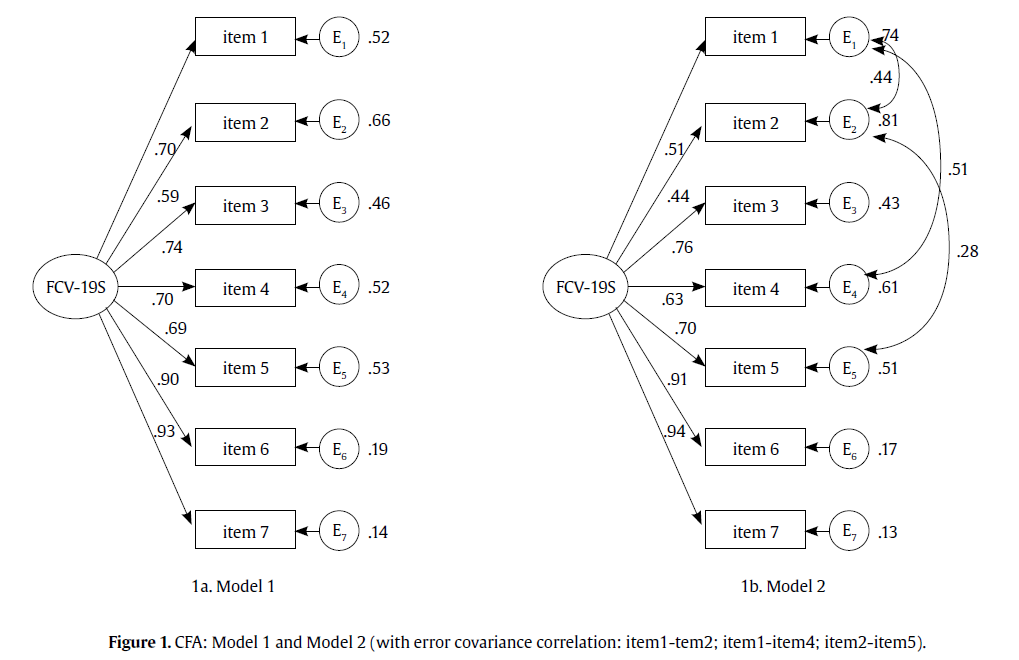
Table 4
3.2. Reliability
Multiple coefficients were estimated to evaluate for internal consistency. Satisfactory results were obtained in all cases, which include Cronbach's Alpha (.79) and McDonald's Omega considering the three correlated errors (.81). With respect to the Test-retest reliability, the value for intraclass correlation was .75, which indicates moderate levels of reliability (Koo & Li, 2016). The corrected item-total correlations oscillated between .47 and .63.
3.3. Convergent Validity
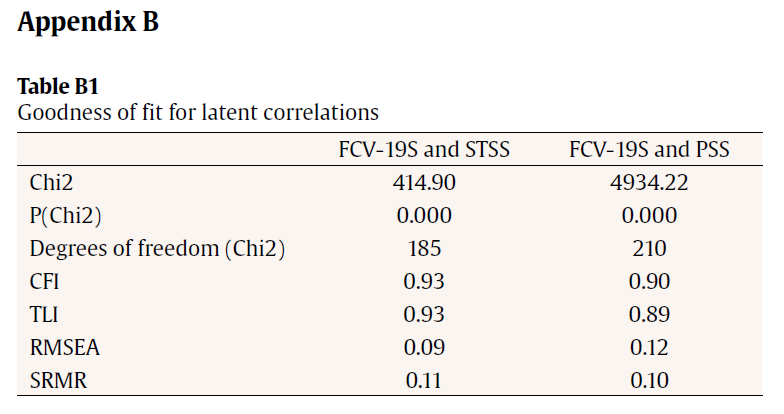
Correlation between total score of FCV-19S and the total scores of Secondary Traumatic Stress Scale and Perceived Stress Scale was found. It was medium, significant and positive, with values of .49 and .48 (p <.001), respectively. Information about the goodness of fit can be found in Appendix B (Table B.1).
3.4. Test-criterion validity evidence
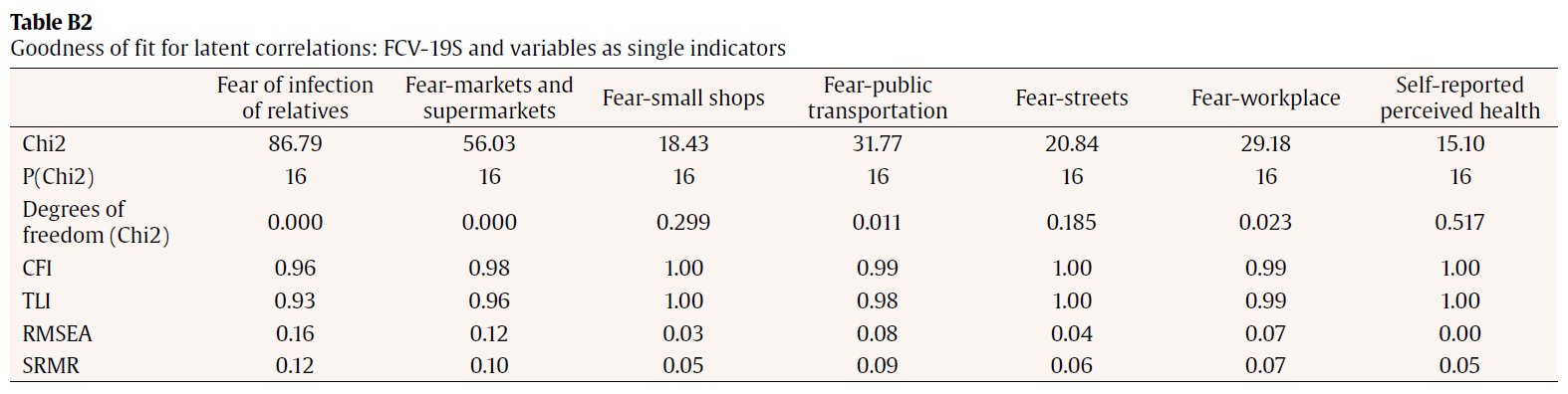
Finally, significant correlations were found between the total score for FCV-19s and the fear of relatives of the participants being infected with COVID-19 (.75) as well as fear of infection of COVID-19 in public places: markets and supermarkets (.47), small shops such as pharmacies and grocery stores (.50), public transportation (.32), streets (.34) and workplace (.46). All these correlations were found to be both significant and positive. Additionally, the fear of COVID-19 also exhibited a significant negative correlation with self-reported perceived health (-.38). Information about the goodness of fit can be found in Appendix B (Table B2).
The contrast of averages detected significant differences (t = -1.46; p = 0.07) between the FCV-19S scores for men (M = 14.54) and women (M = 15.91), with a medium effect size (d = 0.30).
4. Discussion
The present study had the objective of adapting and analyzing the psychometric properties of the FCV-19S (Ahorsu et al., 2020) in a sample of Peruvian professional workers.
The results contribute to the discussion related to the one or two-dimensional nature of the FCV-19S. In line with the majority of previous validations (Alyami et al., 2020; Haktanir et al., 2020; Sakib et al., 2020; Satici et al., 2020; Soraci et al., 2020; Tsipropoulou et al., 2020; Winter et al., 2020), the one-dimensional solution is confirmed. In this sense, our results contrast with those obtained by Masuyama et al. (2020) and by Huarcaya-Victoria et al. (2020), the latter for the Peruvian case, whose results show a bifactor model for the FCV-19S. In contrast to those studies and most validation studies, we used WLSMV as this is the appropriate estimation method for ordinal items. Further studies may test the WLSMV method in larger samples to evaluate if the bifactor model reflects a better factorial structure for the FCV-19S.
In addition to these result, we also found excellent goodness of fit indicators and good standardized factor loading, after the inclusion of three covariance errors in the CFA as performed in previous works (Alyami et al., 2020; Haktanir et al., 2020; Soraci et al., 2020). Regarding reliability, although the obtained alpha (.79) is slightly lower than those found in other studies, this value can still be considered satisfactory, and the same can be said about its corrected item-test correlations and other indicators of reliability, including over time (Test-retest). About its relation to other constructs and in line with previous works (Bitan et al., 2020; Satici et al., 2020), a correlation was found with Secondary Traumatic Stress and Perceived Stress. The scale also presented previously unknown correlations with fear of infection of relatives, fear of infection in public places and self-reported perceived health. To our knowledge, this is the first studies that has performed latent correlations. In that sense, although correlations with other constructs and variables are found, more research is needed since not all goodness of fit indicators suggested a good fit.
Thus, the relevance of studying the fear of COVID-19 goes beyond the necessity of identifying it. Prolonged and excessive sensations of fear can affect functionality and hurt mental health (Tsipropoulou et al., 2020), especially if they are coupled with independent and hard to manage processes such as management of exposure to information in social and news media (Bavel et al., 2020). In this context, the usefulness of studying the fear of COVID-19 encompasses at least three main aspects.
First, its study and use within other investigations would improve the knowledge about the relation between fear of COVID-19 and social functioning so as to adequately direct resources to diminish these levels of fear (Haktanir et al., 2020). The need to make and appropriate and responsible use of social media to quickly and effectively disseminate information has already been suggested (Chan et al., 2020), and these aspects should be experimentally tested to allow for scaled up and more far-reaching solutions. Second, this would allow to identify the need to design focalized interventions in groups with a higher fear and/or vulnerability to infection, or in public places where there exists a higher fear of COVID-19. Third, due to the fact that exaggerated levels of fear of COVID-19 induce irrational thoughts (Ahorsu et al., 2020) and the rejection of initial symptoms in infected subjects (Person et al., 2004), impact interventions regarding fear of COVID-19 may even reduce the incidence of psychological crisis that require hospitalization (Haktanir et al., 2020).
Although the FCV-19S has demonstrated to have good psychometric properties, these results cannot be generalized to the Peruvian population, since we use a small and non-national representative sample, so more studies are required to confirm its psychometric properties. Furthermore, the evaluation of additional indicators of validity (e.g. discriminants) could be considered in future investigations. Also, although women score higher than men, we acknowledge that these results must be further tested in larger samples and complemented with invariance analysis.
This version of the FCV-19S has shown to be valid and reliable, enabling its use and possible contribution to the study of the mental health of the Peruvian population, especially considering the possibility of future waves of COVID-19 spread and the need to understand how fear can influence one's behavior.
Funding. This study received funding from the Consorcio de Investigación Económica y Social (PG-2020-01).
References
Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The Fear of COVID-19 Scale: Development and Initial Validation. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00270-8
Alyami, M., Henning, M., Krägeloh, C. U., & Alyami, H. (2020). Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00316-x
Bavel, J. J. V., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., Crockett, M. J., Crum, A. J., Douglas, K. M., Druckman, J. N., Drury, J., Dube, O., Ellemers, N., Finkel, E. J., Fowler, J. H., Gelfand, M., Han, S., Haslam, S. A., Jetten, J., … Willer, R. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour, 4, 460–471. https://doi.org/10.1038/s41562-020-0884-z
Bitan, D., Grossman-Giron, A., Bloch, Y., Mayer, Y., Shiffman, N., & Mendlovic, S. (2020). Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Research, 289. https://doi.org/10.1016/j.psychres.2020.113100
Brown, T. (2015). Confirmatory Factor Analysis for Applied Research. In The American Statistician (Second edi). The Guilford Press. https://doi.org/10.1198/tas.2008.s98
Chan, A. K. M., Nickson, C. P., Rudolph, J. W., Lee, A., & Joynt, G. M. (2020). Social media for rapid knowledge dissemination: early experience from the COVID-19 pandemic. In Anaesthesia. Blackwell Publishing Ltd. https://doi.org/10.1111/anae.15057
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (Second Edi). Lawrence Erlbaum Associates.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Folkman, S., Lazarus, R. S., Gruen, R. J., & DeLongis, A. (1986). Appraisal, Coping, Health Status, and Psychological Symptoms. Journal of Personality and Social Psychology, 50(3), 571–579. https://doi.org/10.1037/0022-3514.50.3.571
Gao, J., Zheng, P., Jia, Y., Chen, H., Mao, Y., Chen, S., Wang, Y., Fu, H., & Dai, J. (2020). Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE, 15(4). https://doi.org/10.1371/journal.pone.0231924
Guzmán-Yacaman, J. E., & Reyes-Bossio, M. (2018). Revista de Psicologi´a. Revista de Psicología, 36(2), 719–750. http://revistas.pucp.edu.pe/index.php/psicologia/article/view/20033/20036
Haktanir, A., Seki, T., & Dilmaç, B. (2020). Adaptation and evaluation of Turkish version of the fear of COVID-19 Scale. Death Studies, 1–9. https://doi.org/10.1080/07481187.2020.1773026
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
Huarcaya-Victoria, J., Villarreal-Zegarra, D., Podestà, A., & Luna-Cuadros, M. A. (2020). Psychometric Properties of a Spanish Version of the Fear of COVID-19 Scale in General Population of Lima, Peru. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00354-5
Koo, T. K., & Li, M. Y. (2016). A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. Journal of Chiropractic Medicine, 15(2), 155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal, and Coping. Springer Publishing Company.
Masuyama, A., Shinkawa, H., & Kubo, T. (2020). Validation and Psychometric Properties of the Japanese Version of the Fear of COVID-19 Scale Among Adolescents. International Journal of Mental Health and Addiction, 1–11. https://doi.org/10.1007/s11469-020-00368-z
McNeish, D. (2018). Thanks coefficient alpha, We'll take it from here. Psychological Methods, 23(3), 412–433. https://doi.org/10.1037/met0000144
Meda-Lara, R., Moreno-Jiménez, B., Rodríguez, A., Arias, E., & Palomera, A. (2011). Validación mexicana de la Escala de Estrés Traumático Secundario. Psicología y Salud, 21(1), 5–15.
Moreno-Jiménez, B., Garrosa, E., Morante, M. E., Rodríguez, R., & Losada, M. M. (2004). Secondary traumatic stress . Assessment , treatment , prevention. Terapia Psicológica, 22(1), 69–76. http://www.redalyc.org/articulo.oa?id=78522108%0AHow
Ornell, F., Schuch, J. B., Sordi, A. O., & Kessler, F. H. P. (2020). 16. '"Pandemic fear"' and COVID-19: mental health burden and burden strategies. Brazilian Journal Psychiatry, 42, 232–235. https://doi.org/10.1590/1516-4446-2020-0008
Pakpour, A. H., & Griffiths, M. D. (2020). The fear of COVID-19 and its role in preventive behaviors. Journal of Concurrent Disorders, 2(1), 58–63.
Pakpour, A. H., Griffiths, M. D., & Lin, C. Y. (2020). Assessing the psychological response to the COVID-19: A response to Bitan et al. "Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population." In Psychiatry Research (Vol. 290). Elsevier Ireland Ltd. https://doi.org/10.1016/j.psychres.2020.113127
Person, B., Sy, F., Holton, K., Govert, B., Liang, A., Garza, B., Gould, D., Hickson, M., McDonald, M., Mejer, C., Smith, J., Veto, L., Williams, W., & Zauderer, L. (2004). Fear and Stigma: The Epidemic within the SARS Outbreak. In Emerging Infectious Diseases (Vol. 10, Issue 2, pp. 358–363). Centers for Disease Control and Prevention (CDC). https://doi.org/10.3201/eid1002.030750
Perz, C. A., Lang, B. A., & Harrington, R. (2020). Validation of the Fear of COVID-19 Scale in a US College Sample. International Journal of Mental Health and Addiction, 1–11. https://doi.org/10.1007/s11469-020-00356-3
Rajkumar, R. P. (2020). COVID-19 and mental health: A review of the existing literature. Asian Journal of Psychiatry, 52. https://doi.org/10.1016/j.ajp.2020.102066
Reeves, J. (2010). Motivación y emoción. (5ta ed.). México: McGraw-Hill.
Reznik, A., Gritsenko, V., Konstantinov, V., Khamenka, N., & Isralowitz, R. (2020). COVID-19 Fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00283-3
Rubin, G. J., & Wessely, S. (2020). The psychological effects of quarantining a city. In The BMJ (Vol. 368). BMJ Publishing Group. https://doi.org/10.1136/bmj.m313
Sakib, N., Bhuiyan, A. K. M. I., Hossain, S., Al Mamun, F., Hosen, I., Abdullah, A. H., Sarker, M. A., Mohiuddin, M. S., Rayhan, I., Hossain, M., Sikder, M. T., Gozal, D., Muhit, M., Islam, S. M. S., Griffiths, M. D., Pakpour, A. H., & Mamun, M. A. (2020). Psychometric Validation of the Bangla Fear of COVID-19 Scale: Confirmatory Factor Analysis and Rasch Analysis. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00289-x
Satici, B., Gocet-Tekin, E., Deniz, M. E., & Satici, S. A. (2020). Adaptation of the Fear of COVID-19 Scale: Its Association with Psychological Distress and Life Satisfaction in Turkey. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00294-0
Soraci, P., Ferrari, A., Abbiati, F. A., Del Fante, E., De Pace, R., Urso, A., & Griffiths, M. D. (2020). Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00277-1
Tsipropoulou, V., Nikopoulou, V. A., Holeva, V., Nasika, Z., Diakogiannis, I., Sakka, S., Kostikidou, S., Varvara, C., Spyridopoulou, E., & Parlapani, E. (2020). Psychometric Properties of the Greek Version of FCV-19S. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00319-8
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5). https://doi.org/10.3390/ijerph17051729
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., McIntyre, R. S., Choo, F. N., Tran, B., Ho, R., Sharma, V. K., & Ho, C. (2020). A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain, Behavior, and Immunity, 87, 40–48. https://doi.org/10.1016/j.bbi.2020.04.028
Winter, T., Riordan, B. C., Pakpour, A. H., Griffiths, M. D., Mason, A., Poulgrain, J. W., & Scarf, D. (2020). Evaluation of the English Version of the Fear of COVID-19 Scale and Its Relationship with Behavior Change and Political Beliefs. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00342-9
World Health Organization (WHO). (2020a). Alocución de apertura del Director General de la OMS en la rueda de prensa sobre la COVID-19 celebrada el 11 de marzo de 2020. Discursos Del Director General de La OMS. https://www.who.int/es/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020
World Health Organization (WHO). (2020b). WHO Coronavirus Disease (COVID-19) Dashboard. World Health Organization. https://covid19.who.int/
Apendix A
Apendix - B