Original article
Health Anxiety in the Early Phase of COVID-19 Outbreak in Turkey: Investigation of Predictive Variables
Abdi Güngör(a), Halil brahim Sari(b), Esra Asici(b)
- Düzce University, Education Faculty, Departmant of Educational Sciences, Düzce/TURKEY
- Kilis 7 Aralik University, Muallim Rifat Education Faculty, Departmant of Educational Sciences, Kilis/TURKEY
Ansiedad y Estrés, 27 (2021) 74-80
https://doi.org/10.5093/anyes2021a10
https://www.ansiedadyestres.es
Bibliography reference
INFO ARTICLE
Recibido el 11 May 2020
Aceptado el 17 February 2021
Online el 23 September 2021
ABSTRACT
Objective: Health anxiety can be a risk factor for mental health and well-being. People can experience higher levels of health anxiety during pandemic outbreaks because such pandemic outbreaks can cause additional stress and threats. In this sense, people can be more vulnerable to health anxiety during the COVID-19 outbreak. To better understand and overcome health anxiety, it is important to examine factors that affect health anxiety during the COVID-19 outbreak. This study aimed to examine the effects of age, gender, perceived risk, exposure to media, depression, anxiety, and stress on health anxiety during the early phase of the COVID-19 outbreak in Turkey. Materials and Method: The participants included 1473 adults and the data were collected via an online tool. The demographic questions, the Depression Anxiety Stress Scale, and the Short Health Anxiety Scale were used to collect data. Multiple linear regression analysis was implemented to analyze the data using R program. Results: The results showed that anxiety was the strongest positive predictor of health anxiety, following stress, TV News and social media, depression, and risk perception. Age and gender were not found to be significant predictors. Conclusions: This study showed that the significant predictors of health anxiety can escalate health anxiety during the COVID-19 outbreak. The results and limitations are discussed along with implications for future research and intervention and prevention planning.
KEYWORDS
Health anxiety
COVID-19
Pandemic
Outbreak
Risk factors
Ansiedad relacionada con la salud en la fase inicial del brote de COVID-19 en Turquía: Investigación de las variables predictivas
Ansiedad y Estrés, 27 (2021) 74-80
https://doi.org/10.5093/anyes2021a10
https://www.ansiedadyestres.es
Bibliography reference
RESUMEN
Objetivo: La ansiedad relacionada con la salud puede ser un factor de riesgo para la salud mental y el bienestar, particularmente en brotes pandémicos debido a la naturaleza desafiante de la pandemia. En este sentido, las personas pueden ser más vulnerables a la ansiedad relacionada con la salud durante el brote de COVID-19. Para entender mejor y superar la ansiedad de la salud es importante examinar los factores que afectan la ansiedad. Este estudio busca examinar los efectos de género, percepción de riesgo, exposición a medios de comunicación, depresión, ansiedad y estrés sobre la ansiedad de la salud durante la fase temprana del brote de COVID-19 en Turquía. Método: Los participantes incluidos fueron 1473 adultos y la información fue recolectada por medio de una herramienta en Internet. Las preguntas demográficas, la escala DAS y la escala corta de la ansiedad de salud fueron utilizadas para recolectar los datos. El método de regresión lineal múltiple fue aplicado para analizar los datos utilizando el programa R. Resultados: Los resultados mostraron que la ansiedad fue el indicador positivo más importante de la ansiedad de la salud, seguido del estrés, las noticias en televisión y las redes sociales, depresión y la percepción del riesgo. No se encontró que la edad y el género fueran indicadores relevantes. Conclusión: Este estudio reveló que los predictores más importantes de la ansiedad de la salud pueden intensificar la ansiedad de la salud durante el brote de COVID-19. Los resultados y las limitaciones son discutidas junto con las implicaciones para investigaciones futuras y posibles programas de prevención e intervención.
PALABRAS CLAVE
Ansiedad de la salud
Factores de riesgo
Pandemia COVID-19
Introduction
Health anxiety, as one type of anxiety, refers to one's inappropriate and exaggerated fears related to his or her health status (Brand, McKay, Wheaton, & Abramowitz, 2013). People generally experience health anxiety as a result of their misinterpreting information about his or her health status as signs of a serious sickness (Salkovskis, Rimes, Warwick, & Clark, 2002). The level of health anxiety can vary from mild to severe, and have an impact on coping strategies in positive or negative ways (Taylor & Asmundson, 2004). The anxiety can motivate people who have severe diseases to be sensitive to their health; hence they can focus on treatment in advance. In this sense, health anxiety can be functional for people who are at high risk for physical health (Abramowitz, Olatunji & Deacon, 2007). However, it can be dysfunctional when it reaches extreme levels (Wheaton, Abramowitz, Berman, Fabricant, & Olatunji, 2012), and lead people to unnecessary harm their social and occupational lives (Taylor & Asmundson, 2004).
Health anxiety is related to various psychological concerns. Health anxiety has common comorbidity with obsessive-compulsive disorder (Solem et al., 2015), and people who have greater health anxiety are more likely to experience bipolar, agoraphobia, panic disorder, and general anxiety (Sunderland, Newby, & Andrews, 2013). Even more, health anxiety is the main component of hypochondriasis (Aydemir, Kirpinar, Sati, Uykur & Cengisiz, 2013). Hypochondriasis is an extreme form of health anxiety (Abramowitz et al., 2007; Rachman, 2012). Hypochondriacs experience severe and persistent health anxiety because they have an enduring tendency to misinterpret bodily variations and other ambiguous health-related information (Salkovskis et al., 2002).
Health anxiety might emerge when people are under stress, exposed to massive news about contagious diseases, experience some physical symptoms, talk to others about diseases, and witness the sickness of people around (Akkuzu, 2019; Rachman, 2012). A pandemic outbreak is a risk factor that would increase the level of health anxiety. In such outbreaks, people are exposed to great amount of information about contagious diseases, and so feel a threat to their health. Therefore, they may tend to experience higher levels of health anxiety. They can misinterpret somatic reactions such as sweating or higher temperature as being contaminated by the contagious disease. In addition, individuals may get wrong information about the infectiousness of the disease, so their efforts to avoid contagion can lead to dysfunctional behaviors such as obsessive hand-washing (Taylor, 2019). The novel coronavirus (COVID-19) outbreak, which was declared as a pandemic by the World Health Organization (WHO) at the beginning of 2020, can trigger individuals' health anxiety. People can exaggerate any changes in their health status, so they can misinterpret any signs during the COVID-19 outbreak. For example, a simple cough can be interpreted as a symptom of COVID-19. Since health anxiety can be escalated during the COVID-19 outbreak, it can lead to higher levels of psychological issues (Asmundson & Taylor, 2020). Therefore, it is important to examine health anxiety in the COVID-19 outbreak.
Even though it is expected that people experience health anxiety during a pandemic outbreak because of the existence of real threats to human health, there can be factors escalating their health anxiety. Age can be one of those predictive factors of health anxiety in the COVID-19 outbreak. Previous studies on the relationships between age and health anxiety revealed that there was no significant relationship between age and health anxiety (Abramowitz et al., 2007; Wheaton, Berman, Franklin, & Abramowitz, 2010). However, those studies were not conducted in a pandemic outbreak. In a study, it was found that older people can suspect that a possible pandemic influenza can affect them more than other people (Barr et al. 2008). In addition, Cowling et al. (2010) found that older age was generally associated with greater reported use of hygiene measures in the 2009 influenza A (H1N1) pandemic. On the other hand, in a recent study, it was found that people under the age of 30 reported less fear in COVID-19 outbreak (Parlapani et al., 2020). If a pandemic virus has more negative or fatal consequences for people in a certain age group, age can be associated with health anxiety during the pandemic period. Considering that COVID-19 affected older people more severely, both physically and psychologically (Qui et al., 2020), older people are expected to have more fear of being contaminated. Therefore, we hypothesize that age is positively related to higher levels of health anxiety.
Gender can be another factor escalating health anxiety in such pandemic periods. The previous studies showed that there were differences in cognitive, emotional, and behavioral reactions between males and females in a pandemic outbreak. For example, females had higher levels of worry and fear (Prati, Pietrantoni, & Zani, 2011) and tended to comply with preventive measures more than males (Jones & Salathe, 2009; Rubin, Amlôt, Page, & Wessely, 2009) during the swine-flu outbreak. Wang et al. (2020) also found that females were more psychologically affected by COVID-19 during the early phase of the outbreak. In addition, the studies conducted during the COVID-19 period revealed that being female is an important risk factor for health anxiety (Ekiz, Iliman & Dönmez, 2020; Özdin & Bayrak Özdin, 2020). Thus, there are differences in the reactions against a pandemic outbreak between females and males. Because females tend to be more affected psychologically, they can experience higher levels of health anxiety in the COVID-19 outbreak.
Another factor that can trigger health anxiety during pandemic outbreaks can be perceived risk. People's perception of how likely they are contaminated is crucial in terms of the psychological effects of the pandemic. When people have higher levels of perceived risk about the disease, they tend to feel more vulnerable and badly evaluate the consequences of the disease (Taylor, 2019). Prati et al. (2011) found that as the perceived risk of being contaminated by swine-flu was increased, fears and anxiety increased. Similarly, another study conducted during the swine-flu outbreak (Wheaton et al., 2012) found that the perceptions of the probability of being contaminated were related to higher levels of health anxiety. Therefore, as one's perceived risk increases, it is expected that his or her health anxiety to be escalated.
Another concern in a pandemic outbreak is media use. The media provides useful information to the society about the preventive measures in outbreaks, so it can help decrease the risk of contamination (Collinson, Khan, & Heffernan, 2015). However, media use may also lead to developing collective hysteria and fear in society (Wheaton et al., 2012). In a study conducted during avian influenza, watching TV programs about avian influenza was found to be related to higher levels of fear (Van den Bulck & Custers, 2009). Lots of programs and news take place in TVs during the COVID-19 outbreak. People especially follow those news and programs in the early phase of the pandemic to get more information. However, the news on TV and online sources can be confusing or misleading at times. Also, it should be noted that people with higher levels of health anxiety can misinterpret the news on TV and online sources (Salkovskis et al., 2002). Thus, it is expected that there should be a positive relationship between how much people are exposed to TV news and social media about COVID-19 and levels of their health anxiety.
The last factors that we considered as predictive of health anxiety are depression, anxiety, and stress (Koirala, Achary, & Neupane, 2020; Wang et al., 2020). The most basic emotions seen in societies during the pandemic periods are fear and worry. In such periods, people experience serious concerns about the contamination of the virus. These concerns are overwhelming for people, and increase stress. Also, pandemics do not only affect people's physical health, but also have a negative impact on social life, education, and the economy. In this manner, the COVID-19 outbreak caused school closure, restricted traveling, implementing stay-at-home orders, or workplace closures all over the world. It can be difficult for people to adapt to those changes that negatively affect their lives. Although those measures contribute to reducing contamination, they can also increase depression, anxiety, and stress. Especially, social isolation deprives the person of the stress coping mechanisms (Shanmugam, Juhari, Nair, Ken, & Guan, 2020). People can feel depression and hopelessness, and have negative expectations regarding the future, so it can be challenging for them to handle pandemic-related stress. Thus, those feelings can be risk factors for health anxiety. The recent literature has also documented that COVID-19 led to an increase in depression (Huang & Zhao, 2020), anxiety (Shevlin et al., 2020) and stress (Wang et al., 2020) in the society. The literature also showed that depression, anxiety, and stress are related to health anxiety (Olatunji et al., 2009; Wheaton et al., 2012). Thus, we hypothesize that higher levels of depression, anxiety, and stress are related to greater levels of health anxiety.
The increased level of health anxiety in pandemic outbreaks can cause psychological issues (Brand et al., 2013). In this manner, understanding factors affecting health anxiety during the COVID-19 outbreak is crucial for developing preventive and interventive strategies. Thus, this study aimed to investigate the effects of age, gender, and perceived risk, exposure to media, depression, anxiety, and stress on health anxiety during the early phase of the COVID-19 outbreak in Turkey.
Method
Procedures and participants
In this study, we collected the data on the third week of March 2020 and used a snowball sampling method in the data collection. Since people stayed at homes, we collected the data via online tools. First, we created an online form on Google Forms web-based application and sent the electronic link to about 200 Turkish people, and people were encouraged to pass the survey to others. The online form included demographic questions, the Depression Anxiety Stress Scale, and the Short Health Anxiety Scale. The demographic questions were related to gender, age, and perceived risk and the effect of the news and social media. We obtained the required permission from the local Institutional Review Board (IRB) office before the data collection and completed the process in a week. The informed consent form was given to the participants.
The sample of the study consisted of 1638 people from all cities in Turkey. We ran a power analysis to determine whether we had a sufficient sample size. Under medium effect size (e.g., .15), desired statistical power (e.g., .95), and given the number of predictors (e.g., 7), the required sample size was 153. Hence, we had a sufficient number of participants in the study. Before running the data analysis, we removed the outliers violating the assumptions. We retained 1473 cases in the data analysis. After re-checking the required assumptions, we ran multiple linear regression analysis where health anxiety scores were the continuous dependent variable; depression, anxiety, stress, age, perceived risk, and effect of the news and social media were the continuous independent variables; and gender was the categorical independent factor. The purpose of running linear multiple regression analysis was to explore the effects of independent variables on the Turkish sample's level of health anxiety. In the final dataset (N=1473), 1041 (70.7%) participants were female, 432 (29.3%) participants were male, with ages ranging from 18 to 58, the average age was 26 with a standard deviation of 7.88.
Measures
Demographic questions. The first demographic question was gender. There were two options for this item as male and female. The second demographic question was age. This inquiry was in an open-ended format. The third demographic question was risk perception. The item was "Do you feel at risk because of coronavirus?" The inquiry was in a multiple-choice format with three response options as no (0), partially (1), yes (2). The fourth demographic question was regarding news and social media. The item was "To what extent do the news or social media posts related to coronavirus affect you?" The inquiry was in a multiple-choice format with six response options as not at all (0), very little (1), a little (2), some (3), much (4), very much (5).
Depression, Anxiety, and Stress Scale-21 (DASS-21). Lovibond and Lovibond (1995) developed the 41-item version of this survey, and Antony, Bieling, Cox, Enns, and Swinson (1998) developed the 21-item format (short version). Yildirim, Boysan, and Kefeli (2018) adapted the short version into Turkish and validated. The survey aims to measure people's negative emotional situations. The DASS-21 comprises three subscales as depression, anxiety, and stress. Each subscale has seven items, and each item has four response options as 0=never, 1=sometimes, 2=often, 3=always. The Cronbach alpha values in the adaptation study were .89, .87, and .90 for the subscales of depression, anxiety, and stress, respectively. In this study, they were .86, .82, and .87, respectively.
Short Health Anxiety Inventory (SHAI). Salkovskis et al., (2002) developed the English version of this survey, and Aydemir et al. (2013) adapted it into Turkish and validated. The SHAI aims to measure people's mental health (e.g., worry about health, awareness of bodily sensations, fear, etc). The SHAI consists of 18 items and all items have four response options from 0 (no symptoms) to 3 (severe). The SHAI comprises a single dimension meaning that all items measure a single construct of interest. The Cronbach alpha value in the adaptation study was .91, and in this study, it was .86.
Results
Preliminary Analyses
After collecting the data, we first computed total scores for each scale by summing all individual item responses. Then, we checked the assumptions of multiple linear regression analysis such as multicollinearity and multivariate normality. Next, we ran the multiple regression analysis where gender was the categorical predictor; age, depression, anxiety, stress, risk perception, and TV News-social media were continuous predictors; health anxiety was the continuous dependent variable. However, we found that age and gender were not significantly related to health anxiety in the regression model. Additionally, we ran independent samples t-test for the gender to see whether there was a statistical significant difference in the health anxiety scores across males and females. All analyses were completed in R (R Development Core Team 2009-2015), and the source code was provided in the supplementary file.
Table 1
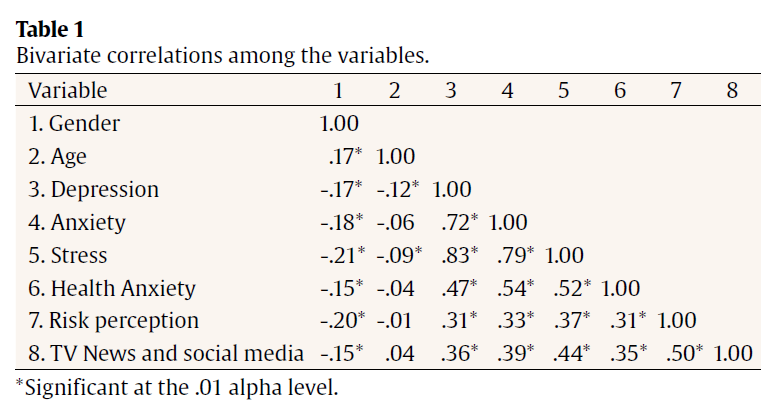
First, we checked the multicollinearity among the independent variables by looking at the bivariate correlations given in Table 1, variance inflation factor (VIF), and tolerance statistics given in Table 2.
Table 2
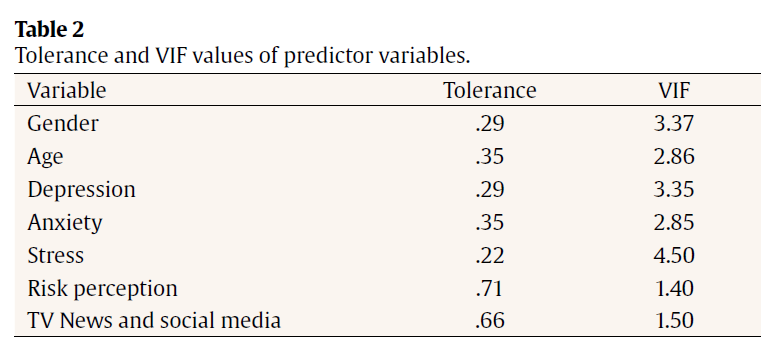
We found that all VIF values were between 1 and 10 (i.e, they were between 1.40 and 4.50 in our study), all tolerance values were higher than .10 (i.e, they were between .22 and .71 in our study), and no bivariate correlation was very high (e.g., higher than .90; i.e, they were between .35 and .83 in our study), indicating no multicollinearity problem (Hair et al., 1998). For the multivariate normality, we ran Mardia test of multivariate normality and checked skewness and kurtosis coefficients and their corresponding statistical significance values. All statistics indicated no non-normality problem (e.g., p>.05).
Statistical Analyses
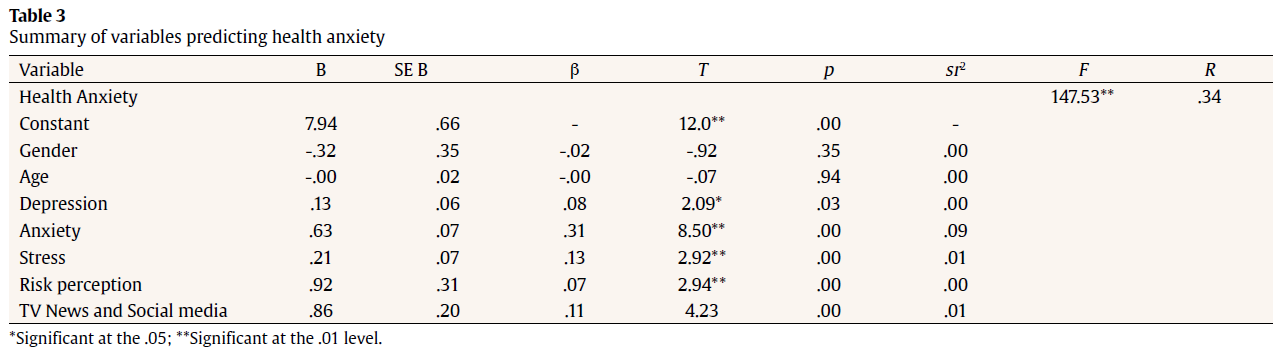
Multiple linear regression using all indicators provided a significant model, F(7, 1459)=105.43, p < .001, R2=.33, meaning that 33% of the variation in health anxiety was explained by the final regression model. The coefficients were given in Table 3. According to Table 3, amongst the variables, anxiety score had the strongest and positive contribution to the health anxiety score (ß=.31, p < .01, sr2=.09), meaning that as the amount of anxiety increased, the health anxiety level of people increased. The stress (ß=.13, p < .02, sr2=.09), TV News and social media (ß=.11, p < .01, sr2=.01), depression (ß=.08, p < .01, sr2=.00) and risk perception (ß=.07, p < .01, sr2=.00) had the second, third, fourth and fifth-highest contributions to the health anxiety score, respectively. All contributions were statistically significant and positively related to health anxiety scores. However, the effects were very small, especially the effects of TV News and social media, depression, and risk perception. Lastly, gender and age were not statistically related to health anxiety, meaning that the changes in gender and age did not meaningfully change the scores on health anxiety. However, based on the independent samples t-test results, there was a statistical difference in the health anxiety scores across males (µ=15.95) and females (µ=18.30), t(1465)=5.71, p<.01. We found that females had greater health anxiety score than males.
Table 3
Discussion
Health anxiety is a risk factor for mental health and well-being (Wheaton et al., 2012; Taylor & Asmundson, 2004). Especially in pandemic outbreaks, health anxiety can be higher because people face a series of threats to their health. Thus, it is important to examine predictive factors of health anxiety to develop prevention and intervention. This study aimed to examine the prediction of age, gender, risk perception, being exposed to TV news and social media, depression, anxiety, and stress on health anxiety in the early phase of COVID-19 outbreak in Turkey. The results showed that the hypothesized factors, except age and gender, significantly predicted health anxiety scores.
More specifically, amongst the variables, anxiety scores (ß=.31) was the strongest predictor of health anxiety scores. The results showed that as participants' anxiety increased, their health anxiety was escalated as well. This result was theoretically expected because health anxiety is defined as one type of anxiety (Brand et al., 2013). People's general anxiety can also be a trigger for health anxiety. In addition, this finding is consistent with the previous studies that showed the positive relationship between anxiety and health anxiety (Olatunji et al., 2009; Wheaton et al., 2012). Thus, people's general anxiety seems like a risk factor for increased levels of health anxiety in the COVID-19 outbreak.
The second positive strongest contribution to health anxiety scores was the level of stress (ß=.13). In other words, higher levels of stress were associated with greater levels of health anxiety. People can be stressed in a pandemic outbreak because, in addition to direct risks to their health, preventive measures can make their lives more challenging. More specifically, to combat COVID-19, various measures had taken place such as school closure, restricted traveling, and implementing stay-at-home orders. Such measures deprive people of the stress coping mechanisms (Shanmugam et al., 2020) and can lead them to feel more stressed. As a result, the individuals experience more health anxiety because they are not able to deal with pandemic-stress effectively. The finding of this study is important because it emphasizes the importance of dealing with stress in the COVID-19 outbreak especially because of the additional distress caused by the nature of pandemic.
TV news and social media had also positive contributions to health anxiety scores (ß=.11). When people were exposed to more TV news and social media about the COVID-19 outbreaks, they had greater levels of health anxiety. During pandemic outbreaks, people demand news and information because an epidemic concerns all society. Therefore, news take a huge place in TV and social media, so people are exposed to a high volume of information. Even though specific news can be a guide for people to prevent the pandemic (Collinson et al., 2015), it can also affect people negatively (e.g. Van den Bulck & Custers, 2009; Wheaton et al., 2012). As the finding of this study showed, TV news and social media in the COVID-19 outbreak were positively associated with an increased level of health anxiety. Therefore, people should put a limit to the TV news and social media use during a pandemic outbreak to combat health anxiety.
The findings of this study also showed that depression (ß=.08) significantly and positively predicted health anxiety even though the effect size was small. When people had higher levels of depression, their levels of health anxiety increased. This finding is consistent with the literature (Koirala et al., 2020; Wang et al., 2020). People suffering from depression believe bad events will happen to them, and so they might think that the coronavirus will contaminate them. Those thoughts and beliefs might trigger health anxiety. Various factors affect people's depression during the COVID-19 pandemic. For example, the aforementioned measures can be challenging for people and may affect their depression. In addition, economic difficulties during the pandemic period lead to negative emotions and thoughts. However, in the current study, factors affecting depression during the COVID-19 pandemic were not assessed. When analyzed together with the other factors, the effect of depression on health anxiety might increase. However when compared to other independent variables, the effect of depression was small but it can still be a risk factor for health anxiety.
The last significant predictive variable was risk perception (ß=.07). Even though its effect size was small as well, risk perception was found to be positively related to health anxiety. Risk perception in this study refers to how likely people believe that they will be contaminated by the coronavirus. When they perceive higher risk, they are more likely to be concerned about their health. Therefore, higher risk perception is associated with higher levels of health anxiety. Previous studies (Prati et al., 2011; Wheaton et al., 2012) also documented that people's perceived risk of contamination was positively related to health anxiety. Thus, it can be useful for people to manage their risk perception to deal with health anxiety.
As can be seen, although the effects of depression, anxiety, stress, being exposed to TV news and social media and risk perception were significant; the effect sizes were quite small. This study was conducted in the early phases of COVID-19 outbreak. The participants may not have had too many negative emotions or thoughts about COVID-19 pandemic at that time. Thus, the level of anxiety, depression and stress of the participants might be lower, and for this reason their risk perception might be lower, too. They might have had optimistic feelings. Even, some people might have been inclined to deny the reality of the COVID-19 outbreak. In the later phases of COVID-19 outbreak, people might have experienced many more negative emotions and thoughts and their risk perception might have increased. In later phases, they might have acquired a better awareness of COVID-19 outbreak. Thus, the effects of those variables on health anxiety might increase in later phases. Also, there might be other factors affecting health anxiety during pandemic period.
This study found that gender was not a significant predictor of health anxiety, contrary to hypotheses. However, the results of independent samples t-test showed that females had higher health anxiety than males. Accordingly, the effect of gender on health anxiety disappeared when the other variables were included in the regression model. All in all, the results supported that being female is a risk factor for health anxiety in COVID-19 pandemic (Ekiz et al., 2020; Özdin & Bayrak Özdin, 2020) and there are gender differences in the reactions to a pandemic (Prati et al., 2011).
This study found that age was not a significant predictor of health anxiety contrary to hypothesis. Older people can suspect that a possible pandemic influenza can affect them more than other people (Barr et al., 2008) and for this reason, they perform recommended behavior during the pandemic (Cowling et al., 2010). On the other hand, young people experience less fear during the outbreak (Parlapani et al., 2020). Thus, we hypothesized that age was associated with health anxiety; however the findings did not confirm our hypothesis. In this study, the average age was 26, and the sample did not include too many elderly people, which can explain this insignificant finding. However, the results of this study supported previous findings indicating no association between age and health anxiety in the COVID-19 pandemic (Ekiz et al., 2020; Özdin & Bayrak Özdin, 2020).
Pandemic outbreaks cause several threats to human health, so people's health anxiety can be escalated in such periods. However, the findings of this study are worthwhile for developing strategies to combat health anxiety. The results showed that higher levels of depression, anxiety, and stress were predictors of health anxiety. Therefore, people need to control and balance their emotional states in such outbreaks. In this context, one of the scopes of public health services should be to provide psychological support for the people during the pandemic periods. Regarding psychological support, individual or group counseling can be provided to individuals with high level of anxiety, depression and stress. Especially, online counseling might be beneficial for those persons. Regarding gender, it was determined that being female was a risk factor for health anxiety during the pandemic period. Therefore, preventive and interventive strategies should specifically target females. It can be helpful to improve females' coping skills. In this sense, psycho-educational studies can be conducted. Another finding was the contribution of TV news and social media on health anxiety. People should be selective and sensitive when following TV news and social media in a pandemic outbreak. However, it should also be noted that this study examined how much people were exposed to TV news and social media, but types of news or information can also be important factors on health anxiety. Therefore, future studies can examine the effects of the types of news and information on health anxiety. In addition, regulations and controls can be made by governments for TV broadcasts during the pandemic periods. Regarding perceived risk, people should have realistic risk perception; hence they could need the right information about the pandemic. Having the right information can help people realistically evaluate the risk factor of being contaminated. In addition, risk perception may be affected by stress. Individuals with high levels of stress may perceive their risk of being contaminated as higher. Stress can affect risk perception first and then health anxiety. In other words, risk perception might have a mediator role in the relation between stress and health anxiety. In the future, the mediator role of risk perception should be investigated. The results of independent samples t-test showed that females had higher health anxiety than males; however in the regression model the effect of gender on health anxiety was not significant. Previous findings showed that females are more vulnerable to pandemics (i.e. Prati et al., 2011; Rubin et al., 2009), so findings regarding females' having higher health anxiety is consistent with the literature. On the other hand, it is known that COVID-19 causes higher risks for older people, but this study was conducted in the early phase of the outbreak. Therefore, people could not have been sufficiently aware of the effects of COVID-19 on older people. In addition, the ages of participants ranged from 18 to 58, which still mostly reflect middle age. It is possible that health anxiety may be higher in elderly population. However, it should be noted that future studies should test this hypothesis.
A limitation of this study is that the sample was predominantly female (7/10 female vs. 3/10 male). This may decrease the validity of the obtained results. A similar study should be conducted with a balanced sample. Age (ranged from 18 to 58, and the mean of 26) was another limitation of the study. As discussed, older people are more vulnerable to COVID-19 than younger ones. Therefore, it could be better to include a wider range of participants' age to better understand the effects of age. Another limitation was that a snowball sampling method to collect data, hence, the generalizability of the results can be limited. This study can be replicated by using a random sampling method. In addition, in the current study, an online survey was implemented. Future studies should use face to face data collection method because internet-based data collection might have some bias. In this study, the administered questionnaire only asks how much people consider that they are being negatively influenced by media information. This question can introduce a bias in the results since people would answer it from their own perspective. This perception may not be realistic since individuals are not always aware of the effects that the media may have on them. In this sense, this variable should have been measured with a better developed instrument. This same aspect must be taken into account regarding the measurement of the risk perception variable. A single question that says "Do you feel at risk because of coronavirus?" is used, regardless of the reasons behind the responses. For example, the health workers might experience more pandemic related anxiety and stress, and for this reason their risk perception might be higher. Future studies should include the variables such as job or chronic illness, and better instruments instead of single questions for these type of measures. This study was based on quantitative research design. In future, in order to gain a deeper understanding, qualitative studies can be conducted. Finally, the course of the COVID-19 outbreak is not the same in all countries. Thus, the studies conducted in different countries can reveal different findings. While evaluating the results of this study, it should be considered that the study was conducted in early phase of COVID-19 outbreak in Turkey.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Abramowitz, J. S., Olatunji, B. O., & Deacon, B. J. (2007). Health anxiety, hypochondriasis, and the anxiety disorders. Behavior Therapy, 38(1), 86-94. doi: 10.1016/j.beth.2006.05.001
Akkuzu, H. (2019). Üniversite ögrencilerinde sosyal zeka ve sosyal sorun çözme becerisinin somatizasyon ve saglik anksiyetesi üzerindeki etkisi (Unpublished master's thesis). Fatih Sultan Mehmet Foundation University, Istanbul, Turkey.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181.
Asmundson, G. J. G. & Taylor, S. (2020). How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. Journal of Anxiety Disorders, 71, 102211. doi: 10.1016/j.janxdis.2020.102211
Aydemir, Ö., Kirpinar, I., Sati, T., Uykur, B., & Cengisiz, C. (2013). Saglik Anksiyetesi Ölçegi'nin Türkçe için güvenilirlik ve geçerlilik çalismasi. Archives of Neuropsychiatry, 50(4), 325-331. doi: 10.4274/npa.y6383
Barr, M., Raphael, B., Taylor, M., Stevens, G., Jorm, L., Giffin, M., & Lujic, S. (2008). Pandemic influenza in Australia: using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infectious Diseases, 8:117. doi:10.1186/1471-2334-8-117
Brand, J., McKay, D., Wheaton, M. G., & Abramowitz, J. S. (2013). The relationship between obsessive compulsive beliefs and symptoms, anxiety and disgust sensitivity, and Swine Flu fears. Journal of Obsessive-Compulsive and Related Disorders, 2(2), 200-206. doi: 10.1016/j.jocrd.2013.01.007
Collinson, S., Khan, K., Heffernan, J.M. (2015) The effects of media reports on disease spread and important public health measurements. PLoS ONE 10(11): e0141423. doi:10.1371/journal.pone.0141423
Cowling, B. J., Ng, D. M., Ip, D. K., Liao, Q., Lam, W. W., Wu, J. T., ... & Fielding, R. (2010). Community psychological and behavioral responses through the first wave of the 2009 influenza A (H1N1) pandemic in Hong Kong. The Journal of Infectious Diseases, 202(6), 867-876.doi: 10.1086/655811
Ekiz, E. Iliman, E., & Dönmez, E. (2020). Bireylerin saglik anksiyetesi düzeyleri ile Covid-19 salgini kontrol algisinin karsilastirilmasi. Uluslararasi Saglik Yönetimi ve Stratejileri Arastirma Dergisi, 6(1), 139-154.
Hair, J. F., Anderson, R. E., Tatham, R. L., & William, C. (1998). Multivariate data analysis (5th. ed.). Englewood Cliffs, NJ: Prentice Hall.
Huang, Y., & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: a web-based cross-sectional survey. medRxiv. (Preprint version). doi: 10.1101/2020.02.19.20025395
Jones, J. H., & Salathe, M. (2009). Early assessment of anxiety and behavioural response to novel swine-origin influenza A(H1N1). PLoS One, 4(12), e:8032. doi:10.1371/journal.pone.0008032
Koirala, J., Acharya, S., & Neupane, M. (2020). Perceived stress in pandemic disaster: A case study from India and Nepal. Available at SSRN 3568388.
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. doi: 10.1016/0005-7967(94)00075-U
Olatunji, B. O., Wolitzky-Taylor, K. B., Elwood, L., Connolly, K., Gonzales, B., & Armstrong, T. (2009). Anxiety sensitivity and health anxiety in a nonclinical sample: Specificity and prospective relations with clinical stress. Cognitive Therapy and Research, 33(4), 416-424. doi: 10.1007/s10608-008-9188-8
Özdin, S. & Bayrak Özdin, S. (2020). Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. International Journal of Social Psychiatry, 66(5), 504-511. doi: 10.1177/0020764020927051
Parlapani, E., Holeva, V., Voitsidis, P., Blekas, A., Gliatas, I., Porfyri, G. N., ... & Bairachtari, V. (2020). Psychological and behavioral responses to the COVID-19 pandemic in Greece. Frontiers in Psychiatry, 11:821. doi: 10.3389/fpsyt.2020.00821
Prati, G., Pietrantoni, L., & Zani, B. (2011). A social-cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Analysis: An International Journal, 31(4), 645-656. doi: 10.1111/j.1539-6924.2010.01529.x
Rachman, S. (2012). Health anxiety disorders: A cognitive construal. Behaviour Research and Therapy, 50(7-8), 502-512. doi: 10.1016/j.brat.2012.05.001
R Development Core Team. (2009-2015). R: A language and environment for statistical computing, reference index (Version 2.2.1). Vienna, Austria: R Foundation for Statistical Computing. http://www.R-project.org, Accessed 10 May 2020.
Rubin, G. J., Amlôt, R., Page, L., & Wessely, S. (2009). Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: A cross-sectional telephone survey. British Medical Journal, 339, b2651. doi:10.1136/bmj.b2651
Salkovskis, P. M., Rimes, K. A., Warwick, H. M. C., & Clark, D. M. (2002). The Health Anxiety Inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychological Medicine, 32(5), 843-853. doi: 10.1017}S0033291702005822
Shanmugam, H., Juhari, J. A., Nair, P., Ken, C. S., & Guan, N. C. (2020). Impacts of COVID-19 pandemic on mental health in Malaysia: A single thread of hope. Malaysian Journal of Psychiatry Ejournal, 29(1).
Shevlin, M., McBride, O., Murphy, J., Miller, J. G., Hartman, T. K., Levita, L., ... & Bennett, K. M. (2020). Anxiety, Depression, Traumatic Stress, and COVID-19 related anxiety in the UK general population during the COVID-19 pandemic. PsyArXiv Preprints (preprint version). doi 10.31234/osf.io/hb6nq
Solem, S., Borgejordet, S., Haseth, S., Hansen, B., Håland, A., & Bailey, R. (2015). Symptoms of health anxiety in obsessive-compulsive disorder: Relationship with treatment outcome and metacognition. Journal of Obsessive-Compulsive and Related Disorders, 5, 76-81. doi: 10.1016/j.jocrd.2015.03.002
Sunderland, M., Newby, J. M., & Andrews, G. (2013). Health anxiety in Australia: prevalence, comorbidity, disability and service use. The British Journal of Psychiatry, 202(1), 56-61. doi: 10.1192/bjp.bp.111.103960
Taylor, S. (2019). The psychology of pandemics: Preparing for the next global outbreak of infectious disease. UK: Cambridge Scholars Publishing
Taylor, S. & Asmundson, G.J.G. (2004). Treating health anxiety: A cognitive-behavioral approach. New York: Guilford.
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. doi: 10.3390/ijerph17051729
Wheaton, M. G., Abramowitz, J. S., Berman, N. C., Fabricant, L. E., & Olatunji, B. O. (2012). Psychological predictors of anxiety in response to the H1N1 (swine flu) pandemic. Cognitive Therapy and Research, 36(3), 210-218. doi: 10.1007/s10608-011-9353-3
Wheaton, M. G., Berman, N. C., Franklin, J. C., & Abramowitz, J. S. (2010). Health anxiety: Latent structure and associations with anxiety-related psychological processes in a student sample. Journal of Psychopathology and Behavioral Assessment, 32(4), 565-574. doi: 10.1007/s10862-010-9179-4
Van den Bulck, J., & Custers, K. (2009). Television exposure is related to fear of avian flu, an ecological study across 23 member states of the European Union. The European Journal of Public Health, 19(4), 370-374. doi: 10.1093/eurpub/ckp061
Yildirim, A., Boysan, M., & Kefeli, M. C. (2018). Psychometric properties of the Turkish version of the Depression Anxiety Stress Scale-21 (DASS-21). British Journal of Guidance & Counselling, 46(5), 582-595. doi: 10.1080/03069885.2018.1442558